8259d473af152443efe6aac33ec11ddf.ppt
- Количество слайдов: 49
 Avian Influenza Shoreland, Inc. April 2006
Avian Influenza Shoreland, Inc. April 2006
 Taipei ‘Wet Market’ China--Backyard Farms
Taipei ‘Wet Market’ China--Backyard Farms
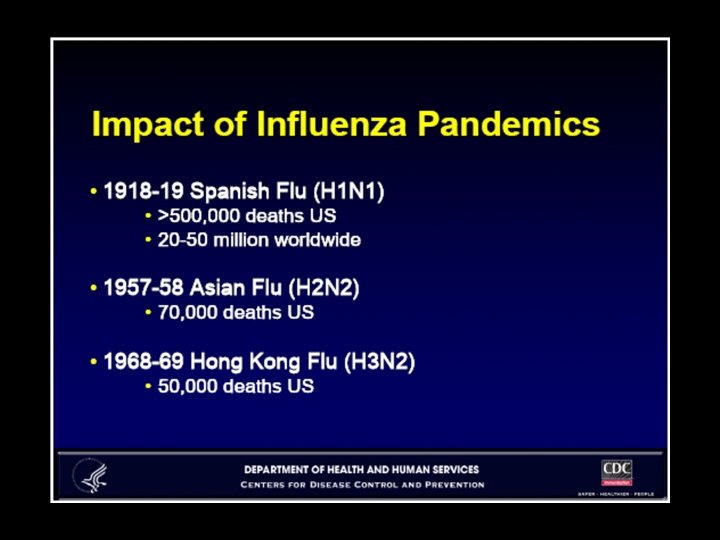
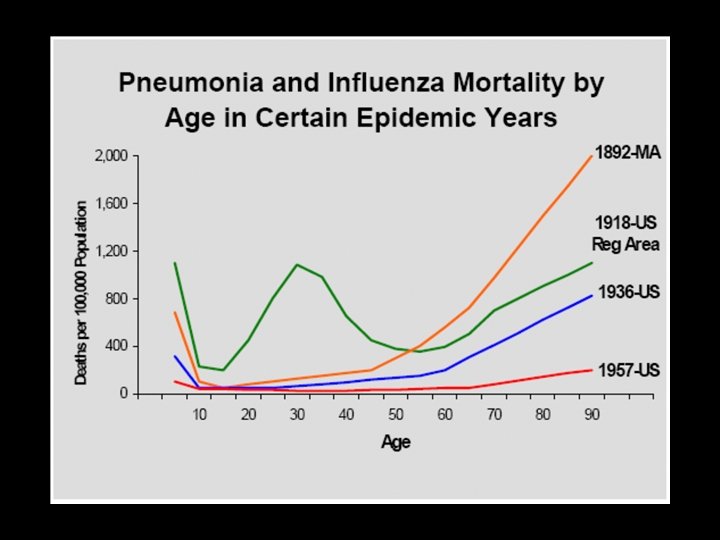
 Pandemic Influenza • Next pandemic inevitable in the near term – Wide agreement by WHO, CDC, others – Current H 5 N 1 “bird flu” or another strain • Worldwide spread within 2 -3 months possible • Initial quarantine may close borders for weeks to months • Highly contagious – Humans have no immunity to new strains • Vaccine availability will lag by months – Insufficient anti-viral drugs currently available • Significant mortality – 1% of world’s population (30 million) died in 1918 pandemic – 1 -2 million died in 1957 & 1968 pandemics – Similar mortality possible if no effective intervention
Pandemic Influenza • Next pandemic inevitable in the near term – Wide agreement by WHO, CDC, others – Current H 5 N 1 “bird flu” or another strain • Worldwide spread within 2 -3 months possible • Initial quarantine may close borders for weeks to months • Highly contagious – Humans have no immunity to new strains • Vaccine availability will lag by months – Insufficient anti-viral drugs currently available • Significant mortality – 1% of world’s population (30 million) died in 1918 pandemic – 1 -2 million died in 1957 & 1968 pandemics – Similar mortality possible if no effective intervention
 H 5 N 1: Confirmed Cases in Humans, Wild Birds, & Poultry (April 4, 2006)
H 5 N 1: Confirmed Cases in Humans, Wild Birds, & Poultry (April 4, 2006)
 H 5 N 1: Confirmed Cases in Humans 192 cases / 109 deaths WHO counts only lab-confirmed cases
H 5 N 1: Confirmed Cases in Humans 192 cases / 109 deaths WHO counts only lab-confirmed cases
 The 2 Mechanisms Whereby Pandemic Influenza Originates
The 2 Mechanisms Whereby Pandemic Influenza Originates
 WHO Pandemic Phases • Inter-Pandemic Period – Phase 1: Animal virus present; no human transmission – Phase 2: Animal virus with features posing risk of human transmission • Pandemic Alert Period – Phase 3: Human infection through animal contact but no human-to-human spread (rarely, spread to a close contact) – Phase 4: Small clusters of limited human-to-human transmission; highly localized – Phase 5: Larger clusters of human-to-human transmission but still localized • Pandemic Period – Phase 6: Worldwide human-to-human infection; increased and sustained transmission in general population
WHO Pandemic Phases • Inter-Pandemic Period – Phase 1: Animal virus present; no human transmission – Phase 2: Animal virus with features posing risk of human transmission • Pandemic Alert Period – Phase 3: Human infection through animal contact but no human-to-human spread (rarely, spread to a close contact) – Phase 4: Small clusters of limited human-to-human transmission; highly localized – Phase 5: Larger clusters of human-to-human transmission but still localized • Pandemic Period – Phase 6: Worldwide human-to-human infection; increased and sustained transmission in general population
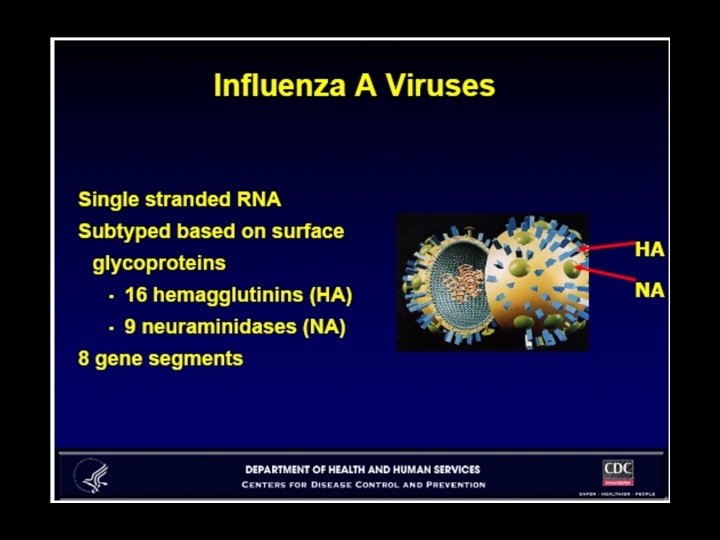
 • Influenza A") Terminology: Pathogenic Avian Serotypes (defined according to disease caused in birds) • Influenza A has many subtypes, classified according to 16 “H” and 9 “N” proteins • Poultry cases – H 5 (generally highly pathogenic) – H 7 (high or low pathogenic varies by strain) – H 9 (always low pathogenic) • Human cases – H 5 (generally severe) – H 7 (mild disease even if highly pathogenic in birds) – H 9 (mild disease; only 3 cases documented)
Terminology: Pathogenic Avian Serotypes (defined according to disease caused in birds) • Influenza A has many subtypes, classified according to 16 “H” and 9 “N” proteins • Poultry cases – H 5 (generally highly pathogenic) – H 7 (high or low pathogenic varies by strain) – H 9 (always low pathogenic) • Human cases – H 5 (generally severe) – H 7 (mild disease even if highly pathogenic in birds) – H 9 (mild disease; only 3 cases documented)
 • Occurs primarily in poultry, waterfowl, or") Avian Influenza A (H 5 N 1) • Occurs primarily in poultry, waterfowl, or other birds • Mammals are susceptible to infection--ingested chicken – Become ill and die – Thus far don’t serve as natural carriers – 2004: pigs (China); tigers & domestic cats (Thailand) – 2006: domestic cat, stone marten (Germany) • Emerged in Asia sometime before 1997 in poultry • 1997 - Mutated into highly pathogenic form – Infected 18 humans (6 deaths) in Hong Kong • 2003 - Re-emerged in poultry – Mutated slightly to “Z” strain • Current wave of bird to human cases since Dec. ‘ 03
Avian Influenza A (H 5 N 1) • Occurs primarily in poultry, waterfowl, or other birds • Mammals are susceptible to infection--ingested chicken – Become ill and die – Thus far don’t serve as natural carriers – 2004: pigs (China); tigers & domestic cats (Thailand) – 2006: domestic cat, stone marten (Germany) • Emerged in Asia sometime before 1997 in poultry • 1997 - Mutated into highly pathogenic form – Infected 18 humans (6 deaths) in Hong Kong • 2003 - Re-emerged in poultry – Mutated slightly to “Z” strain • Current wave of bird to human cases since Dec. ‘ 03
 Reasons for Concern for Pandemic H 5 N 1 • H 5 N 1 can infect many avian and animal species – Facilitates geographic spread • Recombination event is not necessary for a pandemic – 1918 strain pure avian virus that underwent ~10 spontaneous mutations, became infective for humans, and was exceptionally virulent – Several similar mutations present in currently circulating H 5 N 1 virus – NS 1 gene possible virulence factor: one variant of a specific NS 1 gene present in all AI isolates (plus 1918 strain), but no human influenza A
Reasons for Concern for Pandemic H 5 N 1 • H 5 N 1 can infect many avian and animal species – Facilitates geographic spread • Recombination event is not necessary for a pandemic – 1918 strain pure avian virus that underwent ~10 spontaneous mutations, became infective for humans, and was exceptionally virulent – Several similar mutations present in currently circulating H 5 N 1 virus – NS 1 gene possible virulence factor: one variant of a specific NS 1 gene present in all AI isolates (plus 1918 strain), but no human influenza A
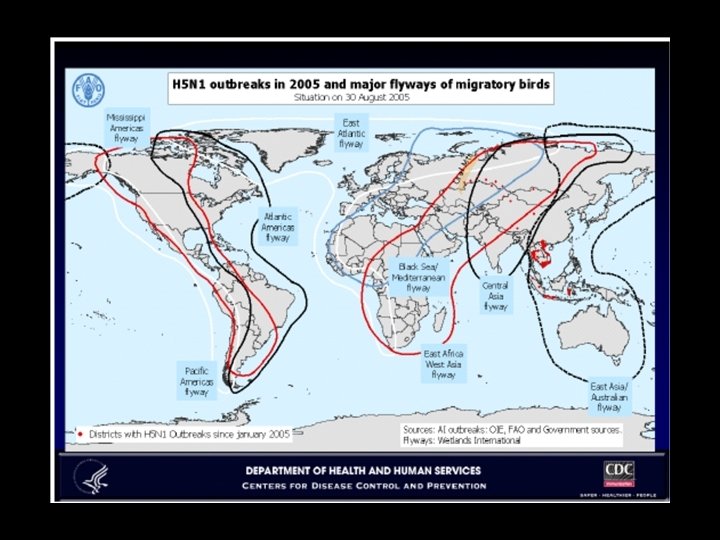
 H 5 N 1 Outbreaks in Birds Countries with H 5 N 1 Outbreaks in 2005 -06 Asia Cambodia China * Hong Kong Indonesia India Kazakhstan Malaysia Mongolia Pakistan (H 5) Russia Thailand Viet Nam Africa Cameroon Egypt Nigeria Burkina Faso Europe Mid-East Azerbaijan Iran** Iraq Israel Albania Austria ** Bosnia & Herzegovina ** Bulgaria ** Croatia Denmark France Germany Greece** Hungary Italy** Poland** Georgia** Jordan Romania Burma (Myanmar) Turkey Serbia & Montenegro Slovakia Slovenia ** Sweden Switzerland** Ukraine United Kingdom** * Cases were reported in birds in the following provinces or autonomous regions during 2005 and/or 2006: Anhui, Guizhou, Hubei, Hunan, Inner Mongolia, Jiangxi, Liaoning, Ningxia, Qinghai, Shanxi, Sichuan, Xinjiang, Xizang (Tibet), and Yunnan. † H 5 confirmed in poultry with further tests pending; however 1 human case has been confirmed as H 5 N 1. ‡ Affected birds exclusively wild/migratory species to date. Countries with outbreaks in 2003 and/or 2004 but not in 2005 -06: Japan, Korea, Laos
H 5 N 1 Outbreaks in Birds Countries with H 5 N 1 Outbreaks in 2005 -06 Asia Cambodia China * Hong Kong Indonesia India Kazakhstan Malaysia Mongolia Pakistan (H 5) Russia Thailand Viet Nam Africa Cameroon Egypt Nigeria Burkina Faso Europe Mid-East Azerbaijan Iran** Iraq Israel Albania Austria ** Bosnia & Herzegovina ** Bulgaria ** Croatia Denmark France Germany Greece** Hungary Italy** Poland** Georgia** Jordan Romania Burma (Myanmar) Turkey Serbia & Montenegro Slovakia Slovenia ** Sweden Switzerland** Ukraine United Kingdom** * Cases were reported in birds in the following provinces or autonomous regions during 2005 and/or 2006: Anhui, Guizhou, Hubei, Hunan, Inner Mongolia, Jiangxi, Liaoning, Ningxia, Qinghai, Shanxi, Sichuan, Xinjiang, Xizang (Tibet), and Yunnan. † H 5 confirmed in poultry with further tests pending; however 1 human case has been confirmed as H 5 N 1. ‡ Affected birds exclusively wild/migratory species to date. Countries with outbreaks in 2003 and/or 2004 but not in 2005 -06: Japan, Korea, Laos
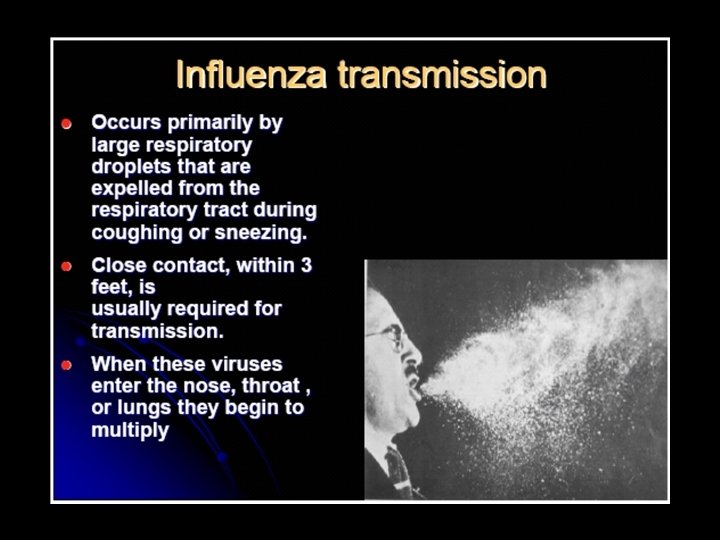
 Transmission • Spread by domestic ducks, poultry, wild migratory birds • Transmitted bird to human through: – Direct contact with sick / infected birds – Surfaces contaminated with droppings, respiratory secretions, ocular secretions – Possibly: eating under-cooked eggs & poultry, duck blood • Human-to-human transmission non-existent or rare with existing H 5 N 1 strain • Incubation period unknown -- 2 -8 days – Pandemic virus (after human adaptation) likely 14 days
Transmission • Spread by domestic ducks, poultry, wild migratory birds • Transmitted bird to human through: – Direct contact with sick / infected birds – Surfaces contaminated with droppings, respiratory secretions, ocular secretions – Possibly: eating under-cooked eggs & poultry, duck blood • Human-to-human transmission non-existent or rare with existing H 5 N 1 strain • Incubation period unknown -- 2 -8 days – Pandemic virus (after human adaptation) likely 14 days
 • Mainly large droplet spread – 3 feet – Emphasis on social") Transmission (cont’d) • Mainly large droplet spread – 3 feet – Emphasis on social distancing • Environmental contact (H 5 N 1 viruses can survive for up to 6 days) • Airborne transmission possible? – Isolate first cases with airborne precautions • Infectious period – 1 day before onset of symptoms to 5 days after in adults and 3 weeks in young children – Big contrast to SARS • Seasonally unclear; winter may be still be higher
Transmission (cont’d) • Mainly large droplet spread – 3 feet – Emphasis on social distancing • Environmental contact (H 5 N 1 viruses can survive for up to 6 days) • Airborne transmission possible? – Isolate first cases with airborne precautions • Infectious period – 1 day before onset of symptoms to 5 days after in adults and 3 weeks in young children – Big contrast to SARS • Seasonally unclear; winter may be still be higher
 H 5 N 1 Clinical -- Symptoms • Initially cannot differentiate from other cases of severe influenza • Presents with fever and influenza-like symptoms, cough, sore throat, rhinitis, muscle aches, headache • Conjunctivitis • Rapid onset of viral pneumonia, ARDS – H 5 N 1 mouse studies indicate diffuse extrapulmonary involvement, macrophage activation, cytokine storm effect • Severest mortality in young adults • Other symptoms, e. g. , severe diarrhea, encephalitis, etc. (see notes)
H 5 N 1 Clinical -- Symptoms • Initially cannot differentiate from other cases of severe influenza • Presents with fever and influenza-like symptoms, cough, sore throat, rhinitis, muscle aches, headache • Conjunctivitis • Rapid onset of viral pneumonia, ARDS – H 5 N 1 mouse studies indicate diffuse extrapulmonary involvement, macrophage activation, cytokine storm effect • Severest mortality in young adults • Other symptoms, e. g. , severe diarrhea, encephalitis, etc. (see notes)
 after becoming") Use of Antivirals • Stand-by treatment – For use (after medical consultation) after becoming ill in an outbreak situation • Dosing as per treatment regimen on “Treatment of Avian Influenza” slide • Prophylaxis – In an outbreak situation, antivirals to be taken as instructed before becoming ill
Use of Antivirals • Stand-by treatment – For use (after medical consultation) after becoming ill in an outbreak situation • Dosing as per treatment regimen on “Treatment of Avian Influenza” slide • Prophylaxis – In an outbreak situation, antivirals to be taken as instructed before becoming ill
 -- recommended • • • Active against H") Types of Antivirals • Oseltamivir (Tamiflu) -- recommended • • • Active against H 5 N 1 in vitro and likely effective in vivo (mice) Shelf life: at least 5 years Supplies limited; not currently in retail stores Until this year 2 million doses per year U. S. current stockpile of antiviral drugs: 5. 5 million treatment courses – an additional 12. 4 million treatment courses of Tamiflu and 1. 75 million treatment courses of Relenza due by Sept 2006 – ? production issues • Zanamivir (Relenza) -- may also be effective • Taken via inhalation - less convenient to use • Amantadine, rimantadine: H 5 N 1 is resistant to these drugs
Types of Antivirals • Oseltamivir (Tamiflu) -- recommended • • • Active against H 5 N 1 in vitro and likely effective in vivo (mice) Shelf life: at least 5 years Supplies limited; not currently in retail stores Until this year 2 million doses per year U. S. current stockpile of antiviral drugs: 5. 5 million treatment courses – an additional 12. 4 million treatment courses of Tamiflu and 1. 75 million treatment courses of Relenza due by Sept 2006 – ? production issues • Zanamivir (Relenza) -- may also be effective • Taken via inhalation - less convenient to use • Amantadine, rimantadine: H 5 N 1 is resistant to these drugs
 Treatment of Avian Influenza • Need to start antiviral treatment in first 48 hours – Reduce mortality / complications • Non-severe cases – 75 mg oseltamivir (Tamiflu) po bid for 5 days • 2 Vietnamese cases with oseltamivir-resistant mutation developing during therapy with death. – Higher dosing may be necessary – Resistant virus not necessarily infectious OR – 10 mg zanamivir (Relenza) inhaled bid for 5 days • Almost none currently available • Severe cases – 150 mg oseltamivir po bid for 7 -10 days – Consider adding inhaled zanamivir (Relenza) – Consider po/IV ribavirin
Treatment of Avian Influenza • Need to start antiviral treatment in first 48 hours – Reduce mortality / complications • Non-severe cases – 75 mg oseltamivir (Tamiflu) po bid for 5 days • 2 Vietnamese cases with oseltamivir-resistant mutation developing during therapy with death. – Higher dosing may be necessary – Resistant virus not necessarily infectious OR – 10 mg zanamivir (Relenza) inhaled bid for 5 days • Almost none currently available • Severe cases – 150 mg oseltamivir po bid for 7 -10 days – Consider adding inhaled zanamivir (Relenza) – Consider po/IV ribavirin
 Prophylaxis of Avian Influenza • Oseltamivir 75 mg po once daily during period of exposure and for 7 -10 days after last exposure – If staying in an area of on-going epidemic with no vaccine available, this could mean taking prophylaxis for 2 months or longer. • Prophylaxis of general public not in current HHS plan
Prophylaxis of Avian Influenza • Oseltamivir 75 mg po once daily during period of exposure and for 7 -10 days after last exposure – If staying in an area of on-going epidemic with no vaccine available, this could mean taking prophylaxis for 2 months or longer. • Prophylaxis of general public not in current HHS plan
 Prevention for the Traveler: Pre-travel • • • Check for any travel restrictions Prohibit travel with a fever to/from H 5 N 1 areas Educate & provide handout on avian influenza Provide travel health kit Supply antivirals (e. g. , oseltamivir) if traveling to H 5 N 1 -affected area (Freedman DO, Leder K. J Trav Med 2005; 12: 36 -44) • Vaccinate with conventional influenza vaccine – Does not protect against H 5 N 1 but may decrease chance of confusing human influenza with H 5 N 1 • Identify in-country health care resources
Prevention for the Traveler: Pre-travel • • • Check for any travel restrictions Prohibit travel with a fever to/from H 5 N 1 areas Educate & provide handout on avian influenza Provide travel health kit Supply antivirals (e. g. , oseltamivir) if traveling to H 5 N 1 -affected area (Freedman DO, Leder K. J Trav Med 2005; 12: 36 -44) • Vaccinate with conventional influenza vaccine – Does not protect against H 5 N 1 but may decrease chance of confusing human influenza with H 5 N 1 • Identify in-country health care resources
 Education: Preventive Measures During Travel • Avoid contact with birds, animal markets / farms, bird droppings or secretions, and potentially contaminated surfaces • Frequent thorough hand washing – Carry and use alcohol hand sanitizer / wipes – Need for paper towels in washrooms – After shaking hands • Ingestion of eggs and poultry that are well cooked • Good respiratory hygiene – When possible, change of airplane seats to avoid travelers with respiratory symptoms; masks when appropriate • Seek early medical consultation for any fever or influenza-like symptoms during or after travel to H 5 N 1 areas
Education: Preventive Measures During Travel • Avoid contact with birds, animal markets / farms, bird droppings or secretions, and potentially contaminated surfaces • Frequent thorough hand washing – Carry and use alcohol hand sanitizer / wipes – Need for paper towels in washrooms – After shaking hands • Ingestion of eggs and poultry that are well cooked • Good respiratory hygiene – When possible, change of airplane seats to avoid travelers with respiratory symptoms; masks when appropriate • Seek early medical consultation for any fever or influenza-like symptoms during or after travel to H 5 N 1 areas
 Travel Kit for H 5 N 1 Areas • • First aid and medical supplies Oral thermometer and probe covers Household disinfectant Disposable gloves and plastic storage bags Alcohol-based wipes / hand sanitizer Masks (2 - or 3 -ply surgical, N 95, others) Consider antivirals (e. g. , oseltamivir)
Travel Kit for H 5 N 1 Areas • • First aid and medical supplies Oral thermometer and probe covers Household disinfectant Disposable gloves and plastic storage bags Alcohol-based wipes / hand sanitizer Masks (2 - or 3 -ply surgical, N 95, others) Consider antivirals (e. g. , oseltamivir)
 Masks • Surgical masks 2 - or 3 -ply • Benefit controversial but may be cultural mandate • N-95 masks • Fit testing required; some limitations but may be good standby protection and useful on airplanes • N-95 or N-100 with exhalation valve • Alternative to N-95 • Exhalation valve increases comfort, temperature, and “wetness” of mask • May be difficult to ensure compliance unless high risk exists
Masks • Surgical masks 2 - or 3 -ply • Benefit controversial but may be cultural mandate • N-95 masks • Fit testing required; some limitations but may be good standby protection and useful on airplanes • N-95 or N-100 with exhalation valve • Alternative to N-95 • Exhalation valve increases comfort, temperature, and “wetness” of mask • May be difficult to ensure compliance unless high risk exists
 Employees/Visitors After Return from H 5 N 1 Areas • Employees/visitors with fever or respiratory illness < 10 days from H 5 N 1 affected area should inform appropriate contact point by telephone and have their illness assessed by the corporate or other health care provider before going into the workplace
Employees/Visitors After Return from H 5 N 1 Areas • Employees/visitors with fever or respiratory illness < 10 days from H 5 N 1 affected area should inform appropriate contact point by telephone and have their illness assessed by the corporate or other health care provider before going into the workplace
 Pandemic Planning Assumptions • Two or more waves in same year or in successive flu seasons • Second wave may occur 3 -9 months later; may be more serious than first (seen in 1918) • Each wave lasts about 6 weeks in a given community
Pandemic Planning Assumptions • Two or more waves in same year or in successive flu seasons • Second wave may occur 3 -9 months later; may be more serious than first (seen in 1918) • Each wave lasts about 6 weeks in a given community
 30% Attack Rate; 10% of Workforce
30% Attack Rate; 10% of Workforce
 Community-based Containment Measures • Slow spread locally; allow for preparation • Slow spread to other communities • Local containment plan – Care, food, services to the isolated or quarantined – Legal preparedness – Flu/fever clinics hotlines • Community communication & cooperation – Voluntary quarantine can work
Community-based Containment Measures • Slow spread locally; allow for preparation • Slow spread to other communities • Local containment plan – Care, food, services to the isolated or quarantined – Legal preparedness – Flu/fever clinics hotlines • Community communication & cooperation – Voluntary quarantine can work
 Pandemic Public Health Measures • Respiratory etiquette – – Cover mouth/nose with sneeze/cough Use tissues Dispose of tissues Immediate hand hygiene • Avoid large gatherings • Surgical masks in public controversial – Social distancing (3 feet) more effective • Symptomatic individuals to wear masks • Snow days; Closure of public places – “Cordon sanitaire”
Pandemic Public Health Measures • Respiratory etiquette – – Cover mouth/nose with sneeze/cough Use tissues Dispose of tissues Immediate hand hygiene • Avoid large gatherings • Surgical masks in public controversial – Social distancing (3 feet) more effective • Symptomatic individuals to wear masks • Snow days; Closure of public places – “Cordon sanitaire”
 Avian Vaccines - Poultry • Avian vaccines used in poultry – Used extensively in several locales, including China – Feb 2004 to Jan 2005: China inoculated 2. 68 billion birds • Not currently thought to be an effective control measure
Avian Vaccines - Poultry • Avian vaccines used in poultry – Used extensively in several locales, including China – Feb 2004 to Jan 2005: China inoculated 2. 68 billion birds • Not currently thought to be an effective control measure
 Avian Vaccines - Human monovalent H 5 N 1 -only vaccines undergoing trials in U. S. and elsewhere – Sanofi: 2 doses were needed at 90 µg given 1 month apart--only 50% of subjects protected (seasonal flu vaccine contains 15 µg) – GSK: Human trials have begun in Europe with low antigen content vaccines with adjuvants – 8 million H 5 N 1 doses on hand by 2/06 (4 million people) – NIH long-term project (Med. Immune) to develop seed virus strains against all known H types, including H 5 N 1 • Egg technology: Long time-line (3 -6 months) for additional doses once decision made, current capacity 5 million doses / month • Cell culture techniques; new investment, several years off • Priority plans: HCWs at top – 50% of the population that are healthy and 2 -64 years at bottom • Current flu vaccines do NOT include avian strains and offer no partial or cross-protection
Avian Vaccines - Human monovalent H 5 N 1 -only vaccines undergoing trials in U. S. and elsewhere – Sanofi: 2 doses were needed at 90 µg given 1 month apart--only 50% of subjects protected (seasonal flu vaccine contains 15 µg) – GSK: Human trials have begun in Europe with low antigen content vaccines with adjuvants – 8 million H 5 N 1 doses on hand by 2/06 (4 million people) – NIH long-term project (Med. Immune) to develop seed virus strains against all known H types, including H 5 N 1 • Egg technology: Long time-line (3 -6 months) for additional doses once decision made, current capacity 5 million doses / month • Cell culture techniques; new investment, several years off • Priority plans: HCWs at top – 50% of the population that are healthy and 2 -64 years at bottom • Current flu vaccines do NOT include avian strains and offer no partial or cross-protection
 Eliminate pandemic virus strain at source? • Recent mathematical models of massive antiviral administration in a localized epidemic situation • “Ring eradication” feasible if: – Low to moderate transmissibility (R 0 < 1. 8) – Chemoprophylaxis of 90% of population within 1 -3 weeks • 1 -3 million courses of oseltamivir needed – Movement restrictions; high compliance
Eliminate pandemic virus strain at source? • Recent mathematical models of massive antiviral administration in a localized epidemic situation • “Ring eradication” feasible if: – Low to moderate transmissibility (R 0 < 1. 8) – Chemoprophylaxis of 90% of population within 1 -3 weeks • 1 -3 million courses of oseltamivir needed – Movement restrictions; high compliance
 Recombined pandemic H 5 N 1 strain vs. SARS • Much more explosively contagious than SARS – Airborne spread – Easy in-flight spread compared to SARS • More difficult to contain with simple quarantine measures than SARS • Will still more rapidly lead to definitive international travel prohibition • May not be seasonal
Recombined pandemic H 5 N 1 strain vs. SARS • Much more explosively contagious than SARS – Airborne spread – Easy in-flight spread compared to SARS • More difficult to contain with simple quarantine measures than SARS • Will still more rapidly lead to definitive international travel prohibition • May not be seasonal