f54020669308ad0d5e27fedc13e2bae7.ppt
- Количество слайдов: 32



Automated External Defibrillators. To What Extent Does the Algorithm Delay CPR? Annals of Emergency Medicine Volume 46, Issue 2, Pages 105 -216 (August 2005) Thomas D. Rea MD, MPH , , Sachita Shah MD, Peter J. Kudenchuk MD, Michael K. Copass MD and Leonard A. Cobb MD From the Department of Medicine, University of Washington (Rea, Shah, Kudenchuk, Copass, Cobb), Public Health, Seattle–King County, Emergency Medical Services Division (Rea), and Seattle Medic One (Copass, Cobb) Seattle, WA 응급의학과 유제성

Introduction 1. Cardiac arrest caused by ventricular fibrillation - in the United States a common cause of cardiovascular death 2. The “chain of survival” outlines opportunities to improve outcomes 1) prompt activation of 9 -1 -1 2) early cardiopulmonary resuscitation (CPR) 3) rapid defibrillation 4) timely advanced life support

Introduction 3. Increasing evidence supports: a critical interaction between CPR and defibrillation so that maximizing CPR may improve survival. 4. Defibrillation- a necessary step for VF 1) after the initial shock current guidelines call for a rhythm reanalysis 2) If ventricular fibrillation persists additional “stacked” shocks, up to 3 total shocks, the shock sequence without an intervening period of CPR. ** A pulse check performed - once defibrillated - or after the third shock of the stack
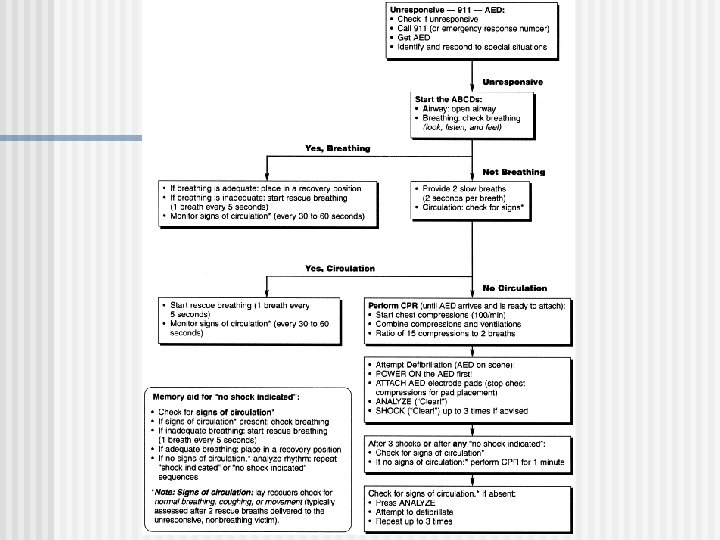

Introduction 5. Each of these activities after shock (rhythm reanalysis, stacked shocks, and pulse check) Changes that minimize or eliminate these activities - provide CPR sooner after shock - increase restoring circulation.

Introduction 6. A single study of nontraditional first responders reported -a pulse never detected with the first pulse check after the initial defibrillating shock. In this experience, a pulse was detected in < 2% of victims 7. To improve the understanding of the balance of potential benefits and risks of these activities ( rhythm reanalyses, stacked shocks, and initial postdefibrillation pulse checks ) in relation to achieving a pulse and initiating CPR.
 the proportion of 1 st , 2 nd and 3")
Introduction 8. determined (1) the proportion of 1 st , 2 nd and 3 rd shocks : 1) resulted in a return of a pulse 2) whether this pulse was detected with the initial postdefibrillation pulse check 3) by defibrillation waveform 4) terminated VF (2) the interval between first shock delivery and initiation of CPR for patients required CPR (3) the interval between termination of ventricular fibrillation and refibrillation
an observational study of victims of ventricular")
Materials and Methods Study Design and Setting 1)an observational study of victims of ventricular fibrillation cardiac arrest 2) treated by EMS first responders 3) from January 1, 1999, through February 29, 2004. The EMS follow the American Heart Association guidelines
 a population of 1. 2 million")
Materials and Methods Study Design and Setting 1) a population of 1. 2 million persons 2) composed of urban, suburban, and rural portions. 3) served by a 2 -tiered EMS system. The first tier : firefighter–emergency medical technicians trained in BLS and defibrillation. The second tier: paramedics trained in advanced life support. First-tier personnel arrive on scene an average of 5 minutes after dispatch and 5 minutes before paramedics

Selection of Participants Excluded - paramedics were on scene before or during the initial shock sequence - because the paramedics 1) trained in rhythm analysis 2) switch the AED to the manual mode.

Data Collection and Processing The EMS of the study county reviews Using a standard data collection form, information was collected about -the amplitude of the ventricular fibrillation waveform before the initial shock - timing of shocks, - the rhythm at 5 and 60 seconds after each shock, - the presence and timing of spontaneous circulation, - CPR - refibrillation

Data Collection and Processing In a blinded assessment of a random subset of 235 rhythms, the interreviewer reliability for rhythm diagnosis : 98. 7% (232/235). the interreviewer reliability for interval from first shock to start of CPR in 40 cases : Agreement was 95% (38/40). Defibrillation : 1) A shock that terminates ventricular fibrillation 2) Results in asystole * considered a successful defibrillation * even though the resulting rhythm does not produce any spontaneous circulation

Data Collection and Processing “shock sequence” 1, 2, or 3 shocks delivered, if necessary, in succession to attempt defibrillation. “stacked” shock - the second or third shock in the shock sequence where defibrillation was not achieved
 the proportion of 1 st, 2 nd")
we used descriptive statistics to determine (1) the proportion of 1 st, 2 nd and 3 rd shocks in the shock sequence that terminated VF (2) the proportion of 1 st, 2 nd and 3 rd shocks in the shock sequence that resulted in a return of a pulse. (3) what proportion of rhythm reanalyses led to a stacked shock (4) what proportion of these stacked shocks produced a pulse (5) the proportion that achieved a pulse as a consequence of rhythm reanalysis (6) Evaluation by AED waveform defibrillation efficacy differ, depending on the defibrillatory waveform (7) the proportion of patients with a pulse detected during the initial postdefibrillation pulse check

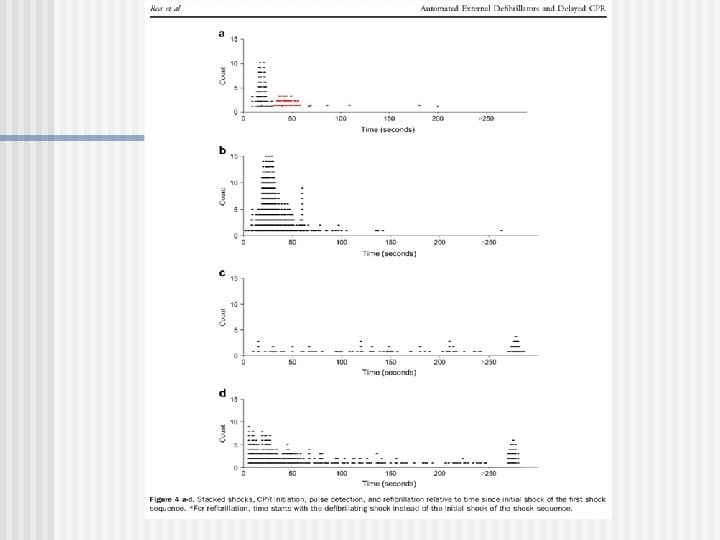
Outcome Measures Scatterplots of the time course the median interval (25 th and 75 th percentiles) - from initial shock to the initiation of CPR - spontaneous circulation, - refibrillation. **** Specifically interested in how the AED algorithm affected the onset of CPR after shock SPSS 11. 0 software for the analyses (SPSS, Inc. , Chicago, IL).

Result

Result
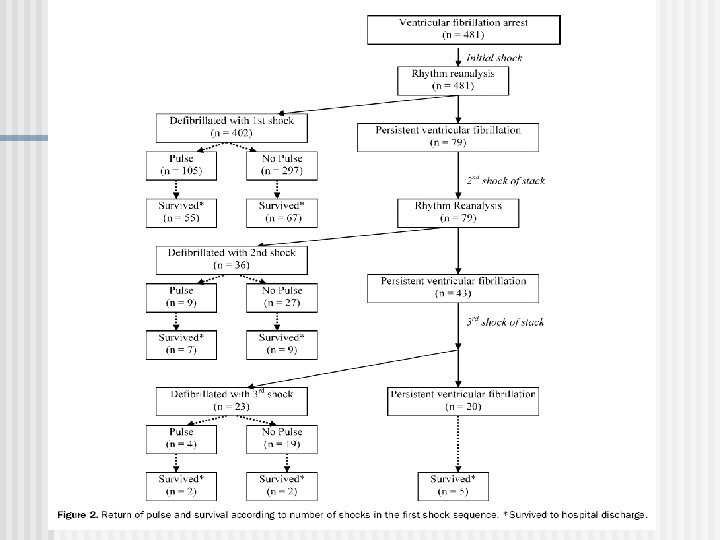

Discussion In cohort with out-of-hospital VF cardiac arrest, the initial shock with AED by first-tier EMS defibrillated : 85% Consequently, the immediate reanalysis of rhythm resulted in a stacked shock : only 15% of the time. The initial shock produced a pulse : 20% a stacked shock produced a pulse : only 10%

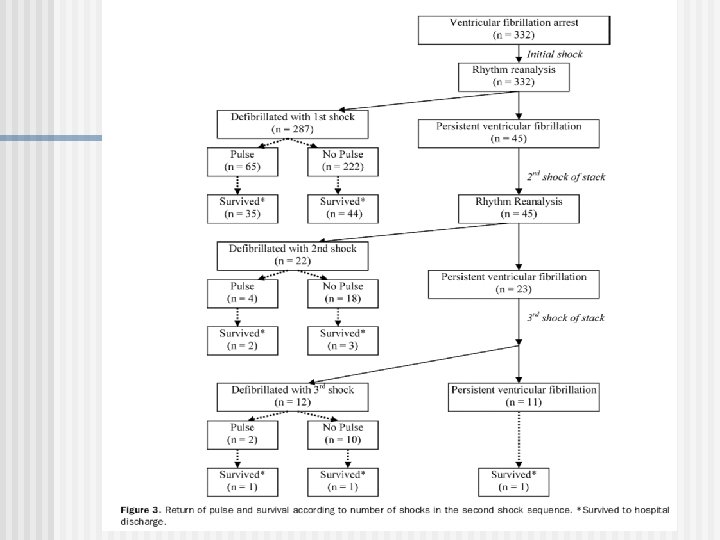
Discussion In Rhythm reanalyses subsequent shocks resulted in a pulse : only 1 of 50 (2. 3% with the first shock sequence (9+4)/(481+79) 1. 6% with the second shock sequence (4+2)/(332+45)) a pulse was detected after the initial shock sequence : ¼ (105/402) Pulse detected during the initial postshock pulse check: only 10% Consequently, the initial postshock pulse check identified : only 1 pulse in 40 (2. 5%)

CPR after the initial shock not initiated until a median of 29 seconds - because of rhythm reanalysis, stacked shocks, and postshock pulse checks Evidence supports 1) the importance of maximizing CPR during VF cardiac arrest. - Interruptions in CPR, delay before shock, and after shock may adversely outcome. 2) support a period of CPR before the initial shock. the mechanism - not entirely clear 3) interruptions in CPR - decrease coronary perfusion and left ventricular filling - a pulse is not produced despite effective defibrillation.
 a dynamic balance between CPR and defibrillation depending on the")
Recent evidence suggests 1) a dynamic balance between CPR and defibrillation depending on the phase of the arrest. 2) During later phases - the importance of CPR increases - delay in defibrillation may be justified. newer waveforms more frequently defibrillate. the initial shock defibrillated 1) the monophasic truncated exponential waveform: 63% 2) monophasic damped sine waveform: 84% 3) biphasic waveforms: 92%

Discussion stacked shocks : only 1/2 of the initial shock produce a pulse A definitive explanation : uncertain stacked shocks exacerbate myocardial stunning and interrupt CPR. The detection of a pulse guides treatment during resuscitation CPR with a pulse -harm, help, or have no survival effect. CPR with pulse -delay other care -injury ( rib or sternal fracture)
a")
Discussion CPR facilitate perfusion patients with a pulse and hypotensive In this study, 1)a pulse detected with the initial postshock pulse check : only 2. 5% 2) though a pulse detected sometime after the initial shock sequence (and before a second shock sequence): 25% Consequently, the postshock pulse checks identified only 1 pulse in 40 cases
 the activities of rhythm reanalyses,")
Discussion What are the implications of the findings? 1) the activities of rhythm reanalyses, 2) stacked shock, 3) initial postshock pulse checks -low yield with regard to the balance between achieving or detecting a pulse and initiating CPR, -Consideration!!! eliminate these activities from the resuscitation algorithm

Discussion The question!!! when to reassess rhythm or pulse. -Although most patients were defibrillated, -Refibrillation was common, >1/2 in VF by 60 sec after the shock sequence, median time to pulse detection after the initial stack: more than 2 minutes

Discussion A finding by the current protocol. These findings indicate - a delay in rhythm analysis and pulse check would likely increase the yield of these activities, though the clinical impact of such changes : uncertain

Discussion CPR was not initiated until approximately 30 seconds after the initial shock. These results suggest AED protocols that prioritize defibrillation Whether resuscitation protocols that limit or eliminate the rhythm reanalyses, stacked shocks, and initial postshock pulse checks will influence survival : uncertain

Discussion Future studies seek !!! define AED protocols provide maximal clinical benefit with regard to the balance between precordial shocks and provision of CPR
 Retrospective, 2) Some cases : AED recordings were not available. 3) Results")
Limitations 1) Retrospective, 2) Some cases : AED recordings were not available. 3) Results are not generalizable - the use of manual defibrillators, - the intervals for reanalysis are shorter. 4) Excluded cases because paramedics were on scene, survival was 39%. 5) No information was available about the functional status of survivors. 6) The investigation took place in a community with a mature EMS system with a relatively quick response time
f54020669308ad0d5e27fedc13e2bae7.ppt