b8bb108df84cdda1470f5118829cccf2.ppt
- Количество слайдов: 79



Autobiographical Memory & Recollective Experience. Martin A. Conway Department of Psychology, University of Durham, England. e-mail: M. A. Conway@durham. ac. uk

What are ‘Autobiographical Memories’?

Autobiographical memories are dynamic transitory mental constructions generated from an underlying multilevel knowledge base which is itself under control of executive processes.

The Self-Memory System

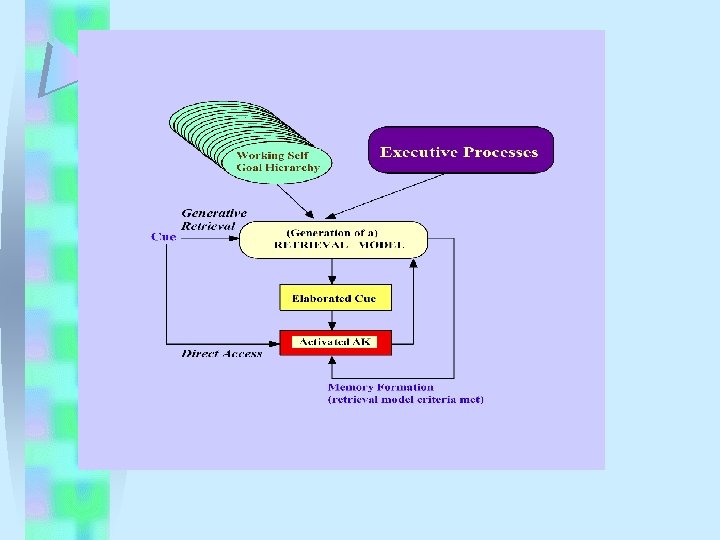
In our model memories are generated within a complex mental system called the “self-memory-system” or SMS. The SMS has two major components: § A knowledge base (in long-term memory). § A set of control processes - which we call the “Working Self”.

The Knowledge Base.

• Autobiographical Knowledge: Conceptual or abstract knowledge about one’s life (sometimes referred to as personal semantic knowledge). • Episodic Memories: Representations of event specific details.

Autobiographical Memories: Are the transitory joining of conceptual autobiographical knowledge with episodic memories.

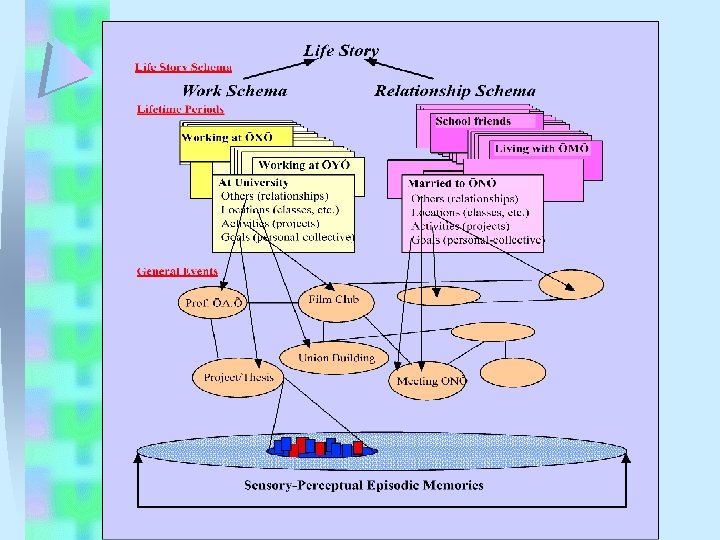
Autobiographical Memory Knowledge Structures in Long. Term Memory

Episodic Memory

Eight Characteristics I. Retain summary records of sensory-perceptual-conceptualaffective processing derived from working memory. II. Represent short time slices, determined by changes in goalprocessing. III. Retain patterns of activation/inhibition over long periods. IV. Represented roughly in order of occurrence. V. They are only retained in a durable form if they become linked to conceptual autobiographical knowledge. VI. They are recollectively experienced when accessed. VII. When included as part of an AM construction they provide specificity. VIII. Neuroanatomically they may be represented in brain regions separate from other AM knowledge networks.

The Working Self

• A complex hierarchy of goals which are all active but which, at any give time, vary in their degree of activation. • A set of self images* and plans derived from the goal hierarchy. *Self images = stories, narratives, actual images, constellations of affect, or all or some combination of these. They are not necessarily conscious but conscious representations might be derived from them.

The Memory Construction Process Generative and Direct Retrieval

Thinking Aloud While Recalling Memories Autobiographical Memory Protocols

Two Protocols

Two Examples of Memories Recalled In the Lab.

Example I: A memory freely recalled by a 54 -year old recalling memories from any point in his life. I remember a bright sunny morning walking down a hill near our house. I had on a red jacket, red shirt, blue jeans, and brown suede boots. I was seventeen. I was going into town and I felt great. . . it was a feeling of being sort of utterly calm, utterly well, a feeling of expectancy: interesting things were about to happen. It was a feeling I don’t think I have had in such a pure form since.

Example II: A response made by a person asked to recall a memory to the (cue) word “Ship”. We were going on holiday to France. I remember that we stayed at a boarding house in Dover and went down to the ferry very early the following morning. My brother and I were wildly excited it was the first time we had been abroad and the first time we had been on a ship of any sorts. I have a vivid memory of looking back at the White Cliffs as the boat pulled out of the harbour - they seemed immensely tall, (Conway, 1996).

The Brain and Memory

A Neuroimaging Study of Memory Retrieval using EEG.

Participants recalled memories to cue words while we monitored changes in brain activation: 1. Prior to retrieval. 2. During retrieval. 3. While a memory was held in mind.

Pre-Retrieval, & Hold Left Anterior Posterior Right

Recollective Experience
.")
Recollective Experience • Recollective experience is the feeling of remembering (a cognitive feeling).

• In autobiographical remembering it occurs when episodic memories are accessed. • Indeed, EMs when accessed always give rise to recollective experience (Wheeler, et al. , 1997, Conway, 2001). • It is associated with images (usually visual), feelings, and a strong sense of the self in the past.

• Moreover when episodic memories enter conscious awareness they ‘hijack’ attention and the system enters what Tulving (1983) called ‘retrieval’ mode.

However, recollective experience although very strongly associated with the conscious representation of EMs can occur: independently of the conscious experience of an EM.

EMs may be accessed but kept out of consciousness (perhaps because of their effect on attention, their cognitive ‘cost’) by control systems, i. e. the working self. But even if they do not enter consciousness they may still trigger recollective experience.

Characteristics of EM: Memory Awareness. Recollective experience does not only occur for EMs but can also occur for false memories (Conway, et al. , 1996; Roediger & Mc. Dermott, 1995) and perhaps in other ways too.

Characteristics of EM: Memory Awareness. • For instance, the preseizure “dream” state experienced by some temporal lobe epileptics often features intense feelings of déjà vu. • Déjà vu as recollective experience for the present.

Characteristics of EM: Memory Awareness. • The temporal lobe epileptics studied by Bancaud, et al. , (1994), mainly with right temporal lobe pathology, had the dream state electrophysiologically induced. • A typical comment from a patient in the dream state was: “The impression of having already done what I am in the process of doing; it seems to me that I have already lived through the entire situation; with a feeling of strangeness and often of fear” NB. The feeling is one of ‘deja vecu’ rather then deja vu.

An experience of déjà vu from Dickens • "At sunset, when I was walking alone, while the horses rested, I arrived upon a little scene, which, by one of those singular mental operations of which we are all conscious, seemed perfectly familiar to me, and which I see distinctly now. There was not much in it. In the blood red light, there was a mournful sheet of water, just stirred by the evening wind; upon its margin a few trees. In the foreground (of a view of Ferrara) was a group of silent peasant girls leaning over the parapet of a little bridge, looking now up at the sky, now down into the water. In the distance a deep dell; the shadow of approaching night on everything. If I had been murdered there in some former life I could not have seemed to remember the place more thoroughly or with more emphatic chilling of the blood; and the real remembrance of it acquired in that minute is so strengthened by the imaginary recollection, that I hardly think I could forget it. " (Dickens, Pictures from Italy).

Characteristics of EM: The Recollective Experience Circuit. • Bancaud, et al. , monitored electrophysiological activation during the dream state in the temporal lobes and limbic system. • They concluded that the dream state was mediated by a circuit located in the medial and lateral regions of the temporal lobes. • Networks in the hippocampus, amygdala, and superior temporal gyrus, have privileged access to this circuit.

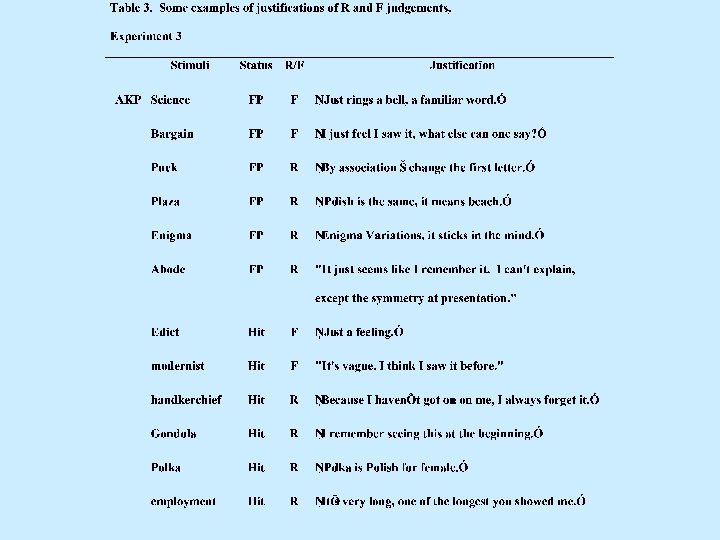
Patients AKP & MA: Chronic Déjà Vu with Recollective Confabulation. • AKP (Moulin, Conway, & James, in prep. ) • 79 year-old, former engineer, university education, bilingual. • Following bilateral atrophy of the temporal lobes and hippocampus (greater on the left than the right), he was referred to a memory clinic (primarily for DAT). • According to his doctor “He does seem to have considerable problems with a sense of déjà vu, both when reading his scientific journals and when reading the newspapers…. . ”

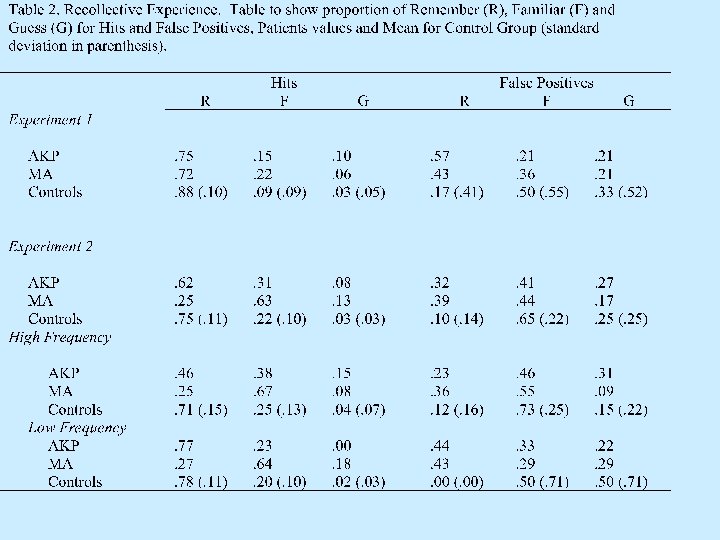
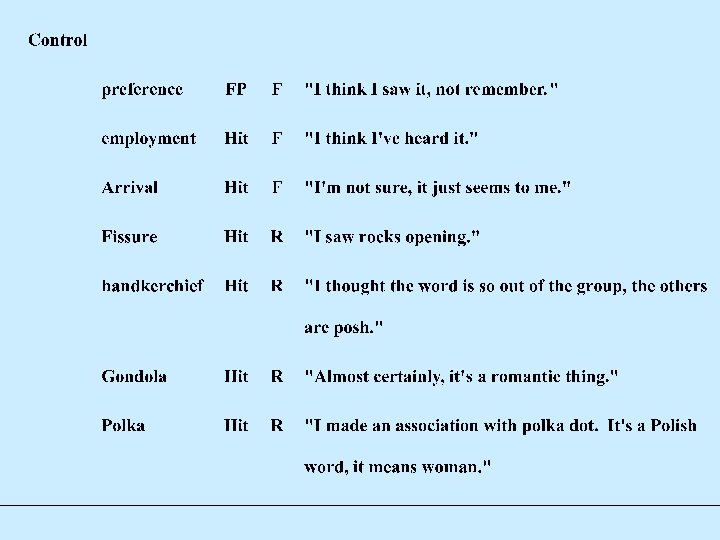
Patient AKP: Chronic Déjà Vu • Intellectually unimpaired, MMSE of 26/28/27, normal fluency, no progressive brain disease, and not diagnosed as DAT. • Quite severe memory problems with impaired free recall, cued recall, and poor recognition with marked overextension of ‘remember’ judgements to false positives. • In his everyday life he constantly experiences déjà vu.

• MA is a 70 year old woman of average intelligence. • Diagnosed as DAT. • She presented to her GP with her husband, who reported that it was as though his wife could predict the future. She was often convinced that things had happened before and complained of persistent feelings of deja vu.

Patients AKP and MA AKP Neuropsychological Examination MA Raw scores Age 80 70 Mini-mental state examination 25 20 NART IQ 115 103 Story Recall Immediate 7 12 Story Recall Delayed 0 0 Visual Recognition – Discrimination Index 9 2 Hopkins Verbal Learning - HVLT Recall 14 14 12 (8) 12 (5) Trails A (sec) 60 182 Trails B (sec) 186 420 FAS (adjusted for education) 30 25 HVLT Recognition – Hits (FPs)

Memory Tests Source Memory Task AKP MA z-scores Hits -3. 27 0. 39 False Positives 4. 19 8. 78 Correct Source Judgements for Hits -3. 25 -15. 80 Correct Recall as a proportion of all attempted -2. 12 -1. 63 Correct Recognition -1. 39 -2. 77 Guesses as a proportion of all responses -0. 39 0. 84 Proportion of incorrect answers that are certain -. 60 -. 04 Correct Recognition -4. 21 -5. 69 Guesses as a proportion of all responses 1. 70 3. 79 Proportion of incorrect answers that are certain -. 49 . 03 Correct Repetitions 0. 77 False Repetitions 22. 27 17. 69 Correct Fame 1. 68 1. 08 Incorrect Fame 4. 71 3. 34 Feeling of Knowing General Knowledge Forced Choice Recognition Face Recognition

Summary • AKP and MA have: False recognition Appropriate confidence judgements Poor recall (but not as bad as recog. ) Recollective experience for the present • They suffer from “Recollective Confabulation” • Moreover they also act upon the (inappropriate) feeling of remembering

Patient AKP: Chronic Déjà Vu • AKP for instance, rarely reads the newspaper believing himself to have already read it. For the same reason he no longer watches television, reads books and letters (the same is true for MA).

Déjà vecu • Christmas cards • TV programmes and newspapers • Tape player • Radio Interview • News Events • Autobiographical information – Classic reduplicative paramnesia or ‘deja vecu’.

Patient AKP: Chronic Déjà Vu • If challenged about how he could have read or seen some item before he usually has a plausible story (confabulation), one not open to contradiction. (When asked, “So what happens next? ” He replied, “How should I know I’ve got a memory problem”). • In short AKP’s chronically overextended feeling of remembering leads him to generate confabulations that ‘explain’ his déjà vu. • This, in turn, leads him to believe that he has already attained goals when he has not, and subsequently to act on these erroneous beliefs.

Groundhog day • Appointments with bank and priest • Moss on roof • Lost items

• We believe that AKP’s and MA’s déjà vecu is a product of fairly constant activation of the recollective experience circuit. • Our view is that this is normal and occurs all the time as EMs are activated automatically by external and internal cues.

• What is abnormal is the failure of control processes to keep the recollective experience from consciousness. • This failure may have occurred in AKP and MA because damage to the medial temporal lobes impaired access from frontal systems but left the recollective experience circuit intact.

Five frontal confabulating patients. Katerina Fotopoulou

Patient Age Sex Neuro Exam Lesion on CT Total R ACA territory Infract Left hemiplegia, visuospatial neglect anosognosia, abnormal pragmatics of communica-tion R internal capsule resion Mild memory impairment, Dysexecutive Syndrome Spontaneous, bizarre, restricted to recent past, specific, constant, reduplicative paramnesia Negative, paranoid, depressive DO 72 F R MCA territory Infract Left hemiplegia, visuospatial neglect, anosognosia Dense R MCA territory infraction Mild memory impairment Dysexecutive Syndrome Spontaneous, bizarre, restricted to recent past, specific, reduplicative paramnesia Negative, paranoid, depressive, anxious, irritable LH 59 M Aco. A Ruptured Normal anosognosia Disorienta-tion Memory impairment Dysexecutive Syndrome Spontaneous, bizarre, not specific, constant or restricted to life-time period Positive, hyperactive, flat to very jocular, wishful, irritable RM 19 M RTA- SAH Normal anosognosia L frontal & bilateral temporal contusions Memory impairment Dysexecutive Syndrome Spontaneous, bizarre, not specific, or restricted to life-time period, but restricted to constantly occurring themes Positive, hyperactive, very jocular, labile, wishful, OT 41 M 2000 -Aco. A Ruptured 2002 - SAH, intraventricula r bleed & Terson’s syndrome Normal, anosognosia Bilateral Prefrontal Cortex lesions Disorientation Severe memory impairment Dysexecutive Syndrome Spontaneous, bizarre, not specific, constant or restricted to life-time period or theme Positive, flat to very jocular, wishful, irritable, labile. AO 87 F Aetiology Neuro. Psychology Confabulation Affect

Examples of true memories, patient’s confabulations, and the experimental confabulations. True memories Confabulations AO: They changed your mattress last week. DO: Your son brought you a present yesterday. RM: You went home last Saturday. LH: Your wife was ill and couldn’t come to see you. Experimental Confabulations AO: Your niece called from London last week. AO: You were changed room at night. AO: A nurse took you to a nursing home in Scotland to stay with her for a while. DO: A male carer took you out in the garden by remote control. DO: A nurse tried to kill you some days ago. She said she hates you. RM: Your father saved a boy during a car accident. RM: You protected your sister from burglars by fighting them off. DO: Your daughter came to see you yesterday. RM: Your sister met with your father recently. LH: You had a case conference last week. OT: You went out with your friends recently. LH: Your surgeon came to tell you, you could smoke as much as you like. LH: You found your car in the hospital parking last week. LH: You went hunting with your friends recently.
. Accurate Memories (N=20) Spontaneous Confabulations (N=20)")
Percentage Recognition of Memories and Confabulations (as memories). Accurate Memories (N=20) Spontaneous Confabulations (N=20) ‘Experimental’ Confabulations (N=20) AO 100 70 30 DO 100 85 30 LH 95 40 25 RM 100 95 35 OT 65 35 35 Patients

• A range of measures were used to assess recollective experience, e. g. presence of imagery, vividness, memory for feelings, recall of associate memories/knowledge, memory of having recalled the ‘memory’ before. • For all 5 patients over 90% of the memories and confabulations were classified as being recollectively experienced. • The ‘experimental memories’ were not, however, associated with imagery, detailed recall, etc.
 of falsely recognised ‘experimental memories’ appeared to be")
• The (relatively low levels) of falsely recognised ‘experimental memories’ appeared to be associated more with a feeling of familiarity than a feeling of recollection.

• The important point is that their own confabulations falsely recognised as true memories were, mostly, recollectively experienced.

• We suggest that when frontal systems are damaged the possibility of recollectively experiencing one’s own fantasies increases. • It may be that inappropriate recollective experience forms the basis of confabulation.

Post Traumatic Stress Disorder With Kevin Meares & Sally Standart, Newcastle Cognitive Behavioural Therapy Unit.
 of parts of the")
Post Traumatic Stress Disorder • In PTSD vivid memories (flashbacks) of parts of the trauma come to mind. • This is often persistent and involuntary. • When a flashback occurs the person may relive (have intense recollective experience) for that part of the trauma.
 and patchy")
• However, PTSD memories are often jumbled (out of temporal order) and patchy with amnesic gaps in between vividly retained details. • Moreover they can contain distortions and errors.

Memory for a Road Traffic Accident A man who drove cars for a living was involved in a road traffic accident. He was a back seat passenger in a car when it was in a high speed collision with another vehicle; activation of the air bags in the front of the car produced a cloud of powder, which he thought at the time was smoke. At the time he could smell petrol and thought the car might ignite and remembers thinking ‘I will be burned alive. ’ His wife was unconscious after the impact and he thought that she had died. He remembered thinking to himself ‘what am I going to do now? ’ as he thought about his future alone without his wife. He has been experiencing terrific guilt about this as it suggests to him that he is a selfish person. In addition, he was an experienced driver and he anticipated the crash, but did not cry out. He felt that he could have averted the crash if he had done this. He experienced intrusive thoughts, such as ‘I should have shouted’ (to warn the driver) and he relived the feeling of guilt he felt when he thought his wife had died, which he believed to be his fault because he did not shout out, (Conway, Meares, & Standart, 2004).

• In this case the intense guilt and anxiety experienced when he recalled his failure to shout was destabilising. So much so that daily activities were disrupted. • However, during therapy, - which included reliving and a visit to the crash site - it became apparent that the way in which the accident occurred (the speed and orientation of the vehicles and their very rapid collision) meant that there could not have been sufficient time to shout a warning. • Once this time expansion distortion in the flashback was recognized the intrusiveness and associated experience of guilt and anxiety diminished.

• From the perspective of our model this is a case in which a memory is distorted, by the working self, to protect the self from a negative cognition (and the revision to self this implies): • namely, that this highly professional driver had not been in control and consequently his belief he always had (virtually ‘omnipotent’) control when driving had to be abandoned.

Memory for a fall 55 year-old man with severe PTSD following a head injury after he fell off an oil rig. When first seen, 2 years after his fall, he had severe depression (BDI =35) and marked PTSD (IES=52).

Flashback Falling down a shaft in the oil rig platform wearing a heavy workmen’s belt. Intensely anxious that he would fall into the water and drown. In reality there was a grid at the bottom of the shaft but it was not present in his flashback in which the sun was very bright and reflected back up the shaft making the grid difficult to see.

In therapy the patient and therapist worked at drawing the grid back into his flashback image. When they achieved this he then suddenly remembered the pain he felt as he hit the grid. This was followed by the realisation that he was alive. BDI =20 and IES =18

• This is a more difficult case for our model. • However, one suggestion is that the lost detail might be an attempt, by the working self, to avoid remembering the pain of the collision with the grid.

9/11 Eye-witness Memory A 21 -year-old man observed the planes going into World Trade Centre from a street close by. Two months later he was referred to the CBT clinic very distressed with an IES of 36 and marked avoidance.

A Flashback with an ‘Observer’ perspective He had a powerful distorted image flashback in which he saw himself high above the ground observing the collision of plane and building. The scene is very peaceful and there is no noise. Although he was able to recognise the implausibility of the ‘memory’ he still maintained it was an actual memory and he experienced it as such. Whenever it intruded into consciousness he felt intense, destabilising, guilt.

Regaining a ‘Field’ perspective In therapy it was realised that this image meant marked avoidance (of the actual memory). Consequently in session 3 he started to practice at imaging coming back to ground and hearing the cries of the crowd standing around him (as they had in real life) and to feel (intense) anger and fear. By session 5 he had regained the original memory with a filed perspective, his IES was down to 10 and the intrusive false memory no longer intruded.

• This type of distortion of perspective is, perhaps, an attempt by the working self to protect against intense negative feelings. • In this case probably intense feelings of foreboding and mounting anxiety occurring at the time.

• We are not claiming that recollective experience forms the basis of PTSD although it clearly must play some role. • Our only claim is that mental representations that are distorted or wholly false when accompanied by recollective experience are experienced by the individual as memories.

Conclusions

• Memories are complex mental representations. • They are constructed from different types of knowledge: conceptual and abstract as well detailed and event-specific. • Episodic memories cause the “feeling of remembering”. • On function of recollective experience might be to signal that a memory is in mind.

• If, however, a memory is not in mind but recollective experience occurs then an illusion of remembering results. • Deja vecu, and perhaps other deja states, are recollective experience in the absence of a memory. • Recollective experience for fantasies and distorted memories allows these to be experienced as memories.

• And, finally, we are currently trying to investigate the feeling states that occur in dreams. • On hypothesis is that experiences in dreams that have a strong feeling of actually happening are points where recollective experience occurs. • In other words the strange feeling of dreams may be, at least in part, the experience of recollection occurring during sleep in a nonconscious state.

Thank You The End
b8bb108df84cdda1470f5118829cccf2.ppt