34deb7efb6636228b4f827cce47f776d.ppt
- Количество слайдов: 45



Aspergillosis Scottish Respiratory Nurses Forum Conference 12 -November-2016 Marie Kirwan
 NAC • The UK's National Aspergillus Centre (NAC) opened")
The National Aspergillosis Centre (NAC) NAC • The UK's National Aspergillus Centre (NAC) opened on May 1 st 2009 • Mycology Reference Centre Manchester (MRCM) processes samples • provides air sampling and mould identification services for domestic and working environments. • NAC clinic Friday's - Chest Clinic 0845 am • Fungal Asthma Clinic (ABPA SAFS) Wednesday's 1. 30 PM pm - Chest Clinic • NAC MDT meeting Thursday's 9 am • Thoracic MDT meeting every Thursday Specialist Thoracic Radiologists • Surgical MDT meeting every three months

NAC Referrals & Outcomes

History of Aspergillus • 1729 - 1 st discovered and catalogued by an Italian biologist – Pier Angelo Micheli • 1815 - 1 st known case of infection 1815 in a Jackdaw • 1842 – 1 st case of human infection in 1842. • 1800’s - 19 th century occupational hazard amongst wig combers allergic disease of the lungs.

What is Aspergillus? • Aspergillus is a fungus whose spores are ubiquitous in the air we breathe • Does not normally cause illness to a healthy individual • Aspergillus can cause disease in weakened immune systems, damaged lungs or allergies • Aspergillosis is a group of diseases which can result from Aspergillus infection and includes • • Allergic Broncho Pulmonary Aspergillosis (ABPA) • Chronic Pulmonary Aspergillosis (CPA) • • Invasive Aspergillosis (IA) Aspergilloma Some asthma patients with very severe asthma may also be sensitised to fungi like Aspergillus (SAFS).

Aspergillus Life Cycle Spores inhaled Germination Mass of hyphae Hyphal elongation & branching
")
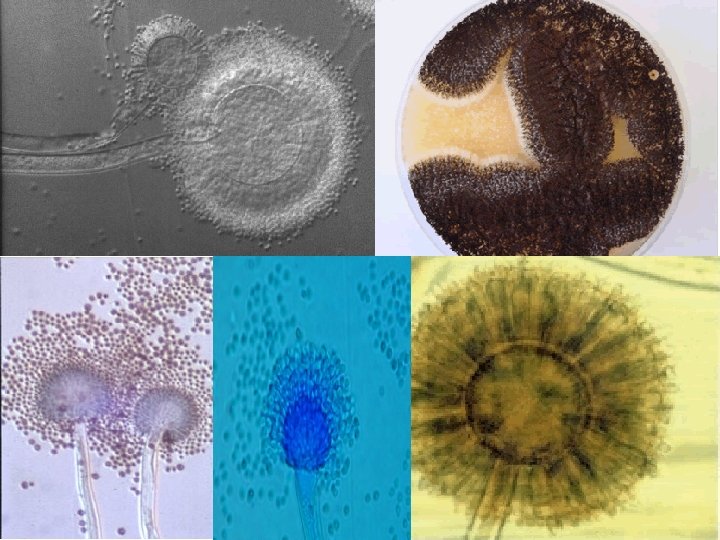
Aspergillus Life Cycle Aspergillus fumigatus spore forming head (Electron micrograph)

Where is Aspergillus species are found in : • Soil • Air; spores may be inhaled • Water / storage tanks in hospitals etc • Food • Compost and decaying vegetation • Fire proofing materials • Bedding, pillows • Ventilation and air conditioning systems • Computer fans
 Subacute IA (1 -3 mo) ABPA Severe asthma with")
Acute invasive (< 4 wks) Subacute IA (1 -3 mo) ABPA Severe asthma with fungal sensitisation Allergic sinusitis Aspergilloma Chronic pulmonary Aspergillus bronchitis Frequency of aspergillosis Aspergillus and aspergillosis Immune deficit Lung damage Allergy-Atopy . After Casadevall & Pirofski, Infect Immun 1999; 67: 3703

Aspergillosis in chronic respiratory diseases Airways/nasal exposure to airborne Aspergillus Invasive aspergillosis • COPD grade III-IV, +/- steroids • ICU - immunoparalysis Chronic aspergillosis (>3 months) • TB and NTM (Non-Tuberculous Mycobacterium) Persistence without disease colonisation of the airways or nose/sinuses • • Sarcoidosis COPD Pneumothorax Pneumonia, RA, asthma, lung surgery Allergic • Allergic bronchopulmonary (ABPA) asthma, CF • Extrinsic allergic (broncho) alveolitis (EAA) • Severe Asthma with fungal sensitisation (SAFS) • Allergic Aspergillus sinusitis (eosinophilic fungal rhinosinusitis)

Prognosis: Comparison of CPA and Aspergillus colonization Ohba et al, Resp Med 2012; 106: 724
 Ig.")
GM test serum Ig. G antibody test Ig. E antibody test Precipitins (serum) Ig. G antibody test Acute invasive GM test Subacute IA other in BAL and Immune compromised ABPA Severe asthma with fungal sensitisation respiratory samples Allergic sinusitis Aspergilloma Chronic pulmonary Aspergillus bronchitis Lung damage Frequency of aspergillosis Aspergillus and aspergillosis Allergy - atopy . After Casadevall & Pirofski, Infect Immun 1999; 67: 3703
 (>3 months) Chronic Cavitary Pulmonary Aspergillosis Aspergilloma Of")
Chronic Disease Chronic Pulmonary Aspergillosis (CPA) (>3 months) Chronic Cavitary Pulmonary Aspergillosis Aspergilloma Of Lung (Fungal Ball) Chronic Fibrosing Pulmonary Aspergillosis
 •")
Chronic Pulmonary Aspergillosis CPA occurs in various forms: • Simple Aspergilloma (Fungal Ball) • Chronic Cavitary Pulmonary Aspergillosis (CCPA) +/ • Chronic Fibrosing Pulmonary Aspergillosis (CFPA) +/CPA occurs in immunocompetent patients unlike invasive aspergillosis Morbidity is significant - both systemic and respiratory symptoms • Haemoptysis • Weight loss • Profound fatigue • Severe shortness of breath • Life-threatening haemoptysis common. Progressive pulmonary fibrosis and loss of lung function common • CPA has a case fatality rate of 20– 33% in the short-term and of 50% over a span of 5 years!

Signs and Symptoms Denning DW et al, Clin Infect Dis 2003; 37: S 265

Who gets Aspergillosis? Aspergillosis affects respiratory & immuno-compromised patients: Chronic • • • Respiratory Disease Cystic fibrosis Chronic Obstructive Pulmonary Disease (COPD) Asthma (ABPA - SAFS) Invasive Aspergillosis • Leukaemia • Chemotherapy patients • HIV or AIDS • Steroids • Transplant patients • Chronic Granulomatous Disease (CGD) • and others…………
")
Chest CT scan with HALO sign (Invasive Disease - Leukaemia)

Chronic Pulmonary Aspergillosis CPA Aspergilloma Chest X-ray

Aspergilloma – Fungal Ball CPA fungal ball is a later stage development
 Allergy to the spores of Aspergillus moulds Predominantly affects")
Allergic Broncho Pulmonary Aspergillosis (ABPA) Allergy to the spores of Aspergillus moulds Predominantly affects patients with • Asthma • CF • Bronchiectasis

Presentation of ABPA • Shortness of breath • Coughing and wheezing • Pulmonary infiltrates that do not respond to antibiotics in asthmatic and CF patients • Cough up plugs of brown coloured mucous • Presence of Aspergillus sensitisation- antibodies serum Total Ig. E >1000 ku/l, Asp Ig. E >0. 4 kua/l, pos skin prick test (ideally both tests) • Can lead to permanent lung damage if left untreated!
 and titre (titre falls with therapy")
Diagnosis of Aspergillosis Investigations: Aspergillus Ig. G (precipitins) and titre (titre falls with therapy and rises with relapse or resistance development) Inflammatory markers, CRP, Plasma Viscosity Total Ig. E (Allergic disease) Aspergillus specific Ig. E (RAST) Sputum – MCS & Fungal sensitivities X-ray CT scan History MRC – Medical Research Council Dyspnoea Score
 Very ill patients: • Save their lives with (usually)")
Objectives of antifungal therapy (CPA) Very ill patients: • Save their lives with (usually) IV and then oral therapy Quite ill patients: • Improve quality of life by minimising symptoms • Prevent further haemoptysis • Stop progression of scarring in the lung • Prevent the emergence of antifungal resistance • Avoid antifungal toxicity Patients with few symptoms • Stop (silent) progression of scarring in the lung • Prevent the emergence of antifungal resistance • Avoid antifungal toxicity

Oral triazole therapy for Chronic Pulmonary Aspergillosis A lower dose advised in those over 70 years, low weight, significant liver disease and those of NE Asian descent who may be slow metabolisers TDM = therapeutic drug monitoring Denning DW et al, Chronic pulmonary aspergillosis – Rationale and clinical guidelines for diagnosis and management. Eur Resp J 2016; 47: 45
 • Itraconazole Levels – random level • Voriconazole Levels –")
Therapeutic Drug Monitoring (TDM) • Itraconazole Levels – random level • Voriconazole Levels – trough level • Posaconazole Levels – record time of last dose Aim is to keep blood concentration at a therapeutic level • Too low can lead to resistance • Too high can result in increased side effects MRCM – and other labs

Drug Management § Itraconazole is available as 100 mg pink and blue capsules with the brand name Sporanox. ® Now generic § Important to take Itraconazole capsules whole with food or an acidic drink, like Coca-Cola. § Itraconazole available as an oral liquid, brand name Sporanox® in a 150 ml bottle, concentration of 10 mg/m. L. § Sugar free cherry flavoured. § It is important to take Itraconazole oral liquid on an empty stomach.

Drug Management § Voriconazole is available as 50 mg or 200 mg tablets Vfend® and generic taken at a dose of 200 mg twice daily, 12 hours apart. § Voriconazole, brand name Vfend® available as an orange flavoured oral liquid of 200 mg/5 m. L. § Important to take Voriconazole tablets whole with food or an acidic drink, like Coca-Cola. § TDM Drug level to adjust dose § (dose range 100 -900 mg daily – split dose)

Drug Management • Posaconazole available as tablets and should be taken at a dose of 400 mg once daily with or without food. • If patients are not eating a lot of food it should be taken 200 mg 4 times daily. • Also available as liquid form 400 mgs twice daily 12 hourly

Monitoring long term azole therapy • LFT abnormalities rare after 6/12 – usually something else • Hypertension with itraconazole • Fatigue and loss of libido • Corticosteroid drug interactions with itraconazole • Skin and skin cancer with voriconazole • Rare cases of myositis and weakness resistance
")
Side effects of Azoles Itraconazole • GI Intolerance • Hepatitis • Peripheral neuropathy (17%) 3 -18 mths after start of drug • Fluid retention • Rash • Hypertension • Cardiac Failure • Headache • Tremor • Insomnia

Side effects of Azoles Voriconazole • Photosensitivity – even trivial light • Visual Disturbance • Peripheral neuropathy (9%) • Poor concentration • Abnormal thinking • Headache • Dry painful lips • Abnormal LFTs • Dry eyes • Tightening feeling of the skin
 • Rash")
Side effects of Azoles Posaconazole • GI Intolerance • Peripheral Neuropathy (1%) • Rash • Headache • Sleep disturbance • Anorexia • Abnormal LFTs • Arrhythmias & palpitations

IV Antifungals • Invasive or resistant disease • Ambisone- 3 weeks course can cause renal impairment. Patients usually have IV saline for an hour prior to the Ambisone. • Ambisone is run over 2 hours or longer if patients are having discomfort or there is evidence of renal deterioration • Micafungin- 4 week course can cause hepatitis (there has been 2 patients where it caused low sodium)
 Agent Oral Itraconazole capsules –")
Drug Management Cost Typical per day daily dose (£) Agent Oral Itraconazole capsules – 1 st Line CPA ABPA Typical duration (range) Typical cost per course 200 mg BID 1. 40 365 £ 512. 94 200 mg BID 13. 33 365 £ 4, 865. 45 Line IA 200 mg BID 82. 83 365 £ 30, 232. 95 Voriconazole capsules – 2 nd Line CPA or 1 st Line IA Posaconazole tablets – Intolerance 150 mg BID 62. 12 365 £ 22, 673. 80 400 mg BID 112. 06 £ 40, 901. 90 Am. Bisome* 3 mg/kg daily 568. 05 21 (14 -30) £ 11929. 05* Am. Bisome 150 mg 3 x wk 1022. 49 per week, £ 145. 66 per day 365 £ 53, 169. 48 50 ug 3 x/wk £ 310. 20 wk 12 weeks £ 3, 722. 40 Itraconazole suspension – Voriconazole capsules – 1 st 2 nd Line CPA or 1 st Intravenous Subcutaneous Gamma-interferon * based on 70 kg person for 21 day course. Ambisome cost per 50 mg vial = £ 113. 61
 and titre •")
Long Term Management Blood tests • Serial Aspergillus Ig. G (precipitins) and titre • Inflammatory markers, CRP, Plasma Viscosity • Total Ig. E (Fungal Asthma) • Aspergillus specific Ig. E (RAST) (Fungal Asthma) Sputum • Microscopy • Sputum – sensitivities Asp PCR Radiology • X-ray • CT scan History – crucial for assessment for toxicity MRC – Medical Research Council Dyspnoea Score St Georges Respiratory Questionnaire Research Avoidance to known sources of Aspergillus spores

How to avoid Aspergillus Pulmonary infections can be prevented by avoiding sources of Aspergillus spores: • Smoking • Bedside humidifiers • Animal stables • Hay • Mulch • Rotten plants, • Compost piles, • Wood & bark chips • Construction sites

Denning DW et al, Chronic pulmonary aspergillosis – Rationale and clinical guidelines for diagnosis and management. Eur Resp J 2016; 47: 45 -68.
 • Questionnaires, sensitisation")
• 7, 104 young adults in 13 countries (11 Europe) • Questionnaires, sensitisation to Alternaria and Cladosporium, assessment of homes, asthma evaluation (metacholine challenge). • New onset asthma the key output (n=355) • Follow up 8. 7 (5. 9 -11. 7) years. • Risk ratio for new asthma = 1. 46 (water damage) and 1. 3 (indoor moulds). • Correlation with water damage and mould in the house Norback D, Occup Environ Med 2013; 70: 325 -31.
 & Institute for Specialist Surveyors and Engineers (ISSE)")
Damp Homes National Aspergillosis Centre (NAC) & Institute for Specialist Surveyors and Engineers (ISSE) http: //nacpatients. org. uk/damp_general Dr Graham Atherton 2016

Asthma and fungus Interactions • Fungal and damp exposure at home increases the risk of asthma • Dampness and fungus at home increase asthma exacerbations • Thunderstorm asthma • Some occupational asthma linked to fungal exposures • [Link between fungi and extrinsic allergic alveolitis] • Fungal sensitisation linked to severe asthma • Antifungal therapy reduces asthma severity in most patients with ABPA and SAFS

What should I do? • Identify source of water and stop it • Occasionally it is a leak from plumbing, roof, guttering • Usually it is excessive humidity caused by a combination of: • Normal daily living (cooking, washing, breathing!) • Poor house design and lack of ventilation • If neither of these options is true seek further advice (Environmental Health Officer or www. isse. org. uk ) Dr Graham Atherton 2016

www. aspergillus. org. uk 18 years Over 1 M pages read monthly in >125 countries Supported by the Fungal Infection Trust – 25 year anniversary 2016 New section on drug interactions which you can search very quickly + app for iphones android (search antifungal interaction) 691 interactions were rated as minor, 919 moderate and 381 severe, = 2216 recorded interactions

GAFFI Global Action Fund for Fungal Infection VISION is to reduce illness and death associated with fungal diseases worldwide - a “hidden crisis”. MISSION is to improve the health of patients suffering from serious fungal infections through better patient care, improved access to o diagnostics and treatment, and by provision of educational resources to health professionals. WHY GAFFI? • Fungal Infections are neglected diseases worldwide • Globally, > 300 million people of all ages estimated to suffer from a serious fungal infection every year • Of these, over 1. 66 million people are estimated to die • In comparison, deaths from malaria and tuberculosis are 600, 000 and 1, 540, 000 respectively

On behalf of the National Aspergillosis Centre Team Thank You
34deb7efb6636228b4f827cce47f776d.ppt