
Aortic Valve Disease Normal Aortic Valve




- Размер: 26.3 Mегабайта
- Количество слайдов: 68
Описание презентации Aortic Valve Disease Normal Aortic Valve по слайдам
Aortic Valve Disease
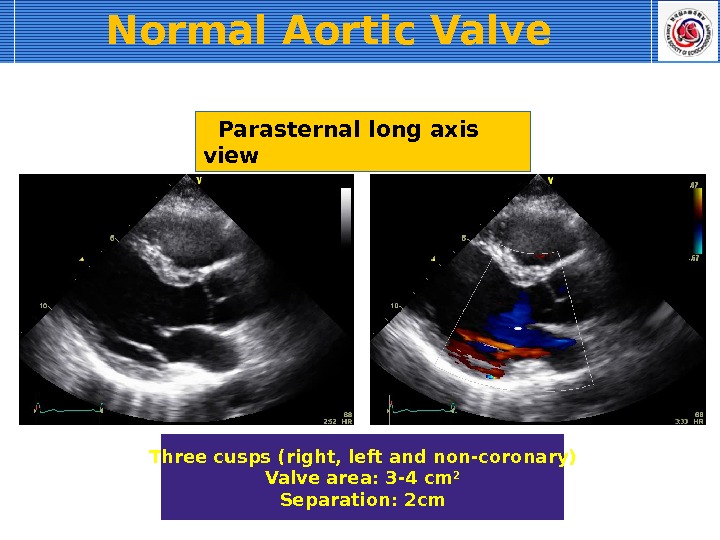
Normal Aortic Valve Parasternal long axis view Three cusps (right, left and non-coronary) Valve area: 3 -4 cm 2 Separation: 2 cm
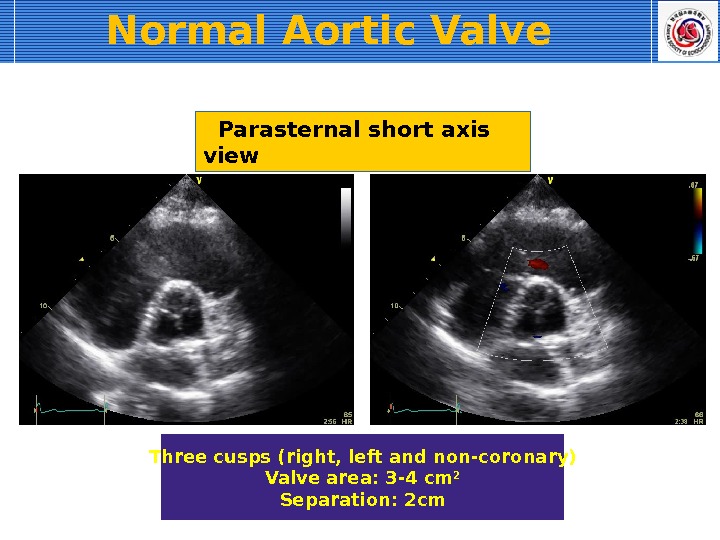
Parasternal short axis view Three cusps (right, left and non-coronary) Valve area: 3 -4 cm 2 Separation: 2 cm. Normal Aortic Valve
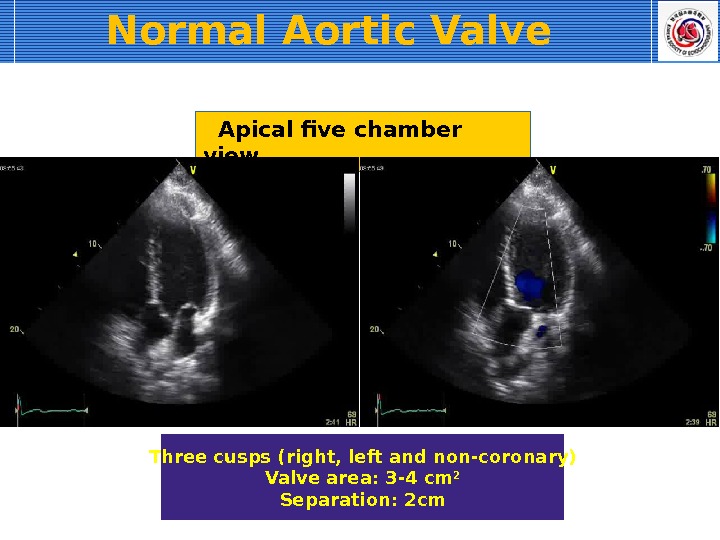
Apical five chamber view Three cusps (right, left and non-coronary) Valve area: 3 -4 cm 2 Separation: 2 cm. Normal Aortic Valve
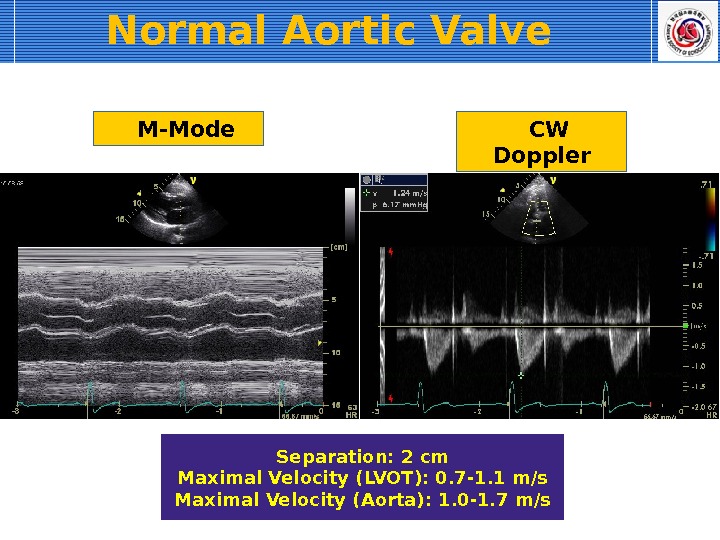
M-Mode Separation: 2 cm Maximal Velocity (LVOT): 0. 7 -1. 1 m/s Maximal Velocity (Aorta): 1. 0 -1. 7 m/s CW Doppler. Normal Aortic Valve
Congenital Anomaly Unicuspid valve Bicuspid valve Quadricuspid valve
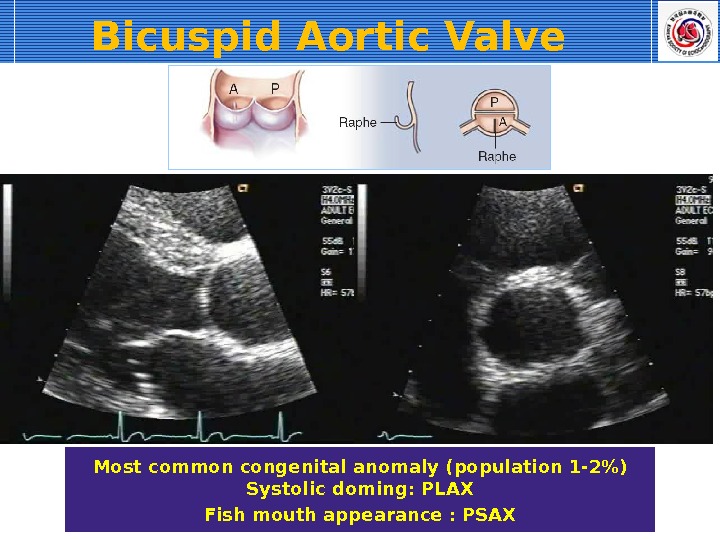
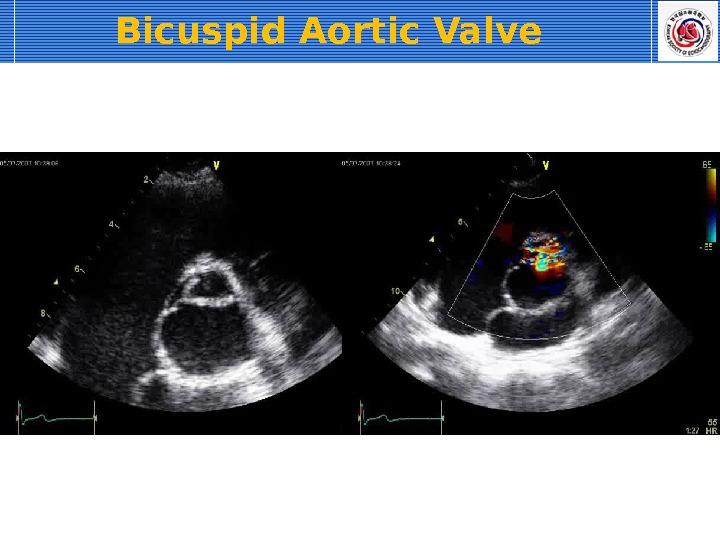
Bicuspid Aortic Valve Most common congenital anomaly (population 1 -2%) Systolic doming: PLAX Fish mouth appearance : PSAX
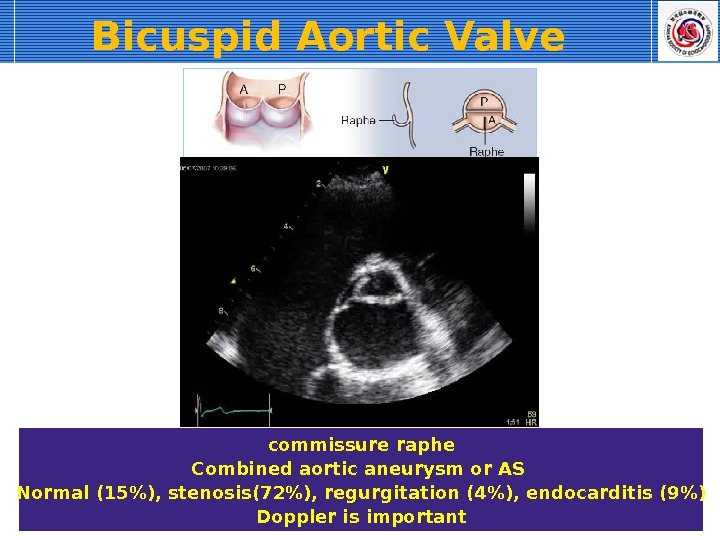
commissure raphe Combined aortic aneurysm or AS Normal (15%), stenosis(72%), regurgitation (4%), endocarditis (9%) Doppler is important. Bicuspid Aortic Valve
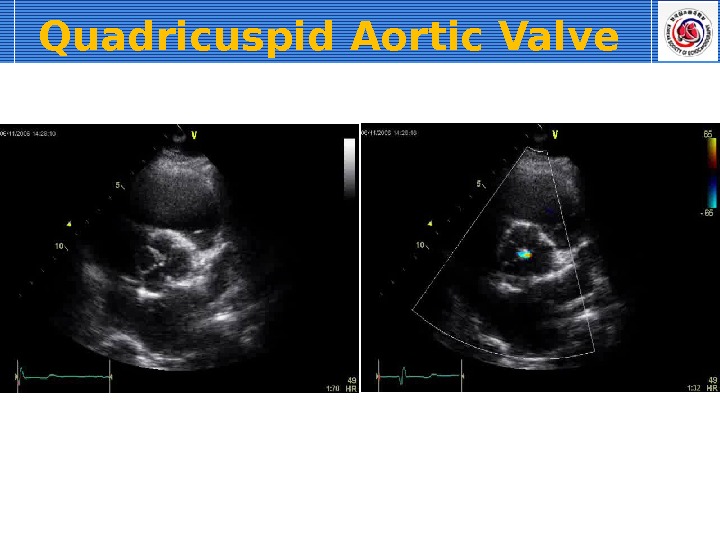
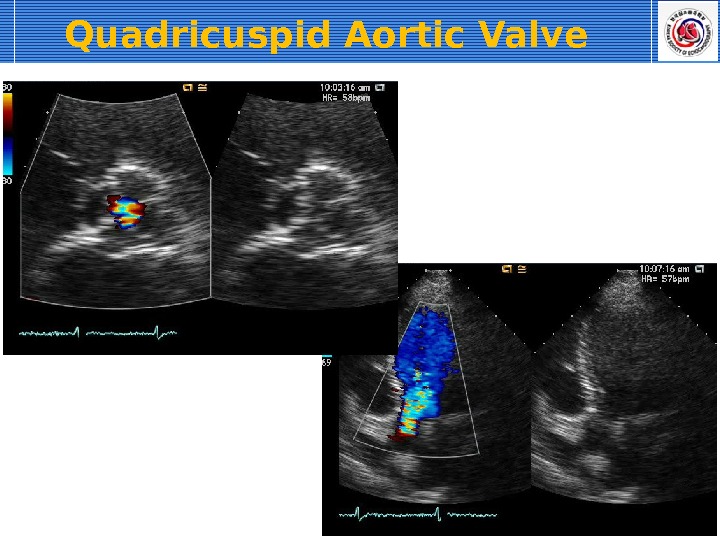
Quadricuspid Aortic Valve
Aortic Stenosis
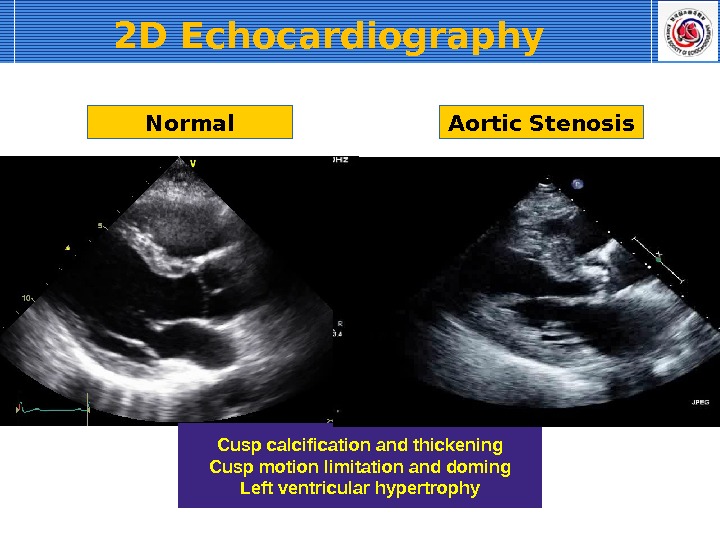
2 D Echocardiography Normal Aortic Stenosis Cusp calcification and thickening Cusp motion limitation and doming Left ventricular hypertrophy
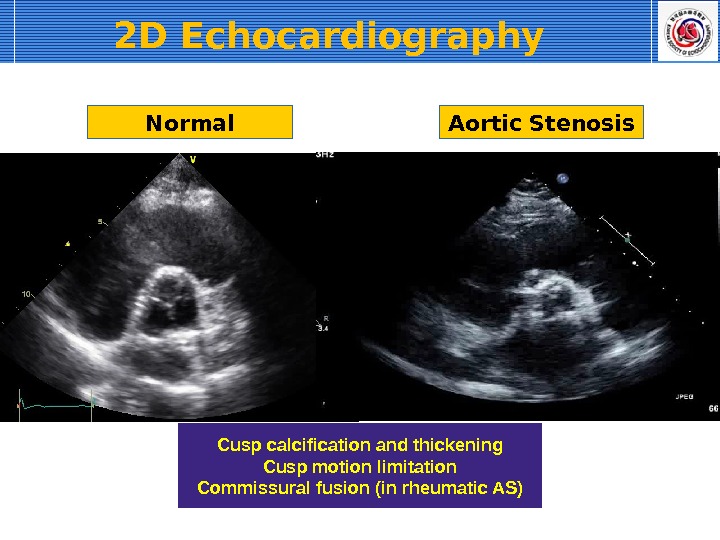
Normal Aortic Stenosis Cusp calcification and thickening Cusp motion limitation Commissural fusion (in rheumatic AS)2 D Echocardiography
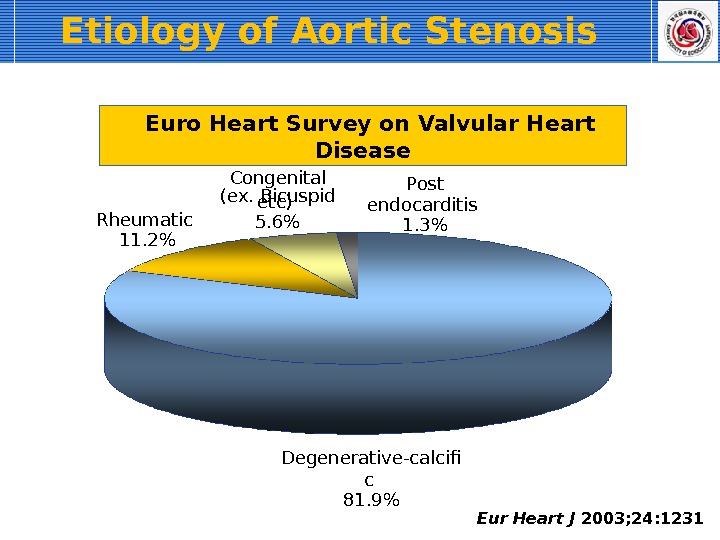
Etiology of Aortic Stenosis Eur Heart J 2003; 24: 1231 Degenerative-calcif c 81. 9%Rheumatic 11. 2% Congenital (ex. Bicuspid etc) 5. 6% Post endocarditis 1. 3% Euro Heart Survey on Valvular Heart Disease
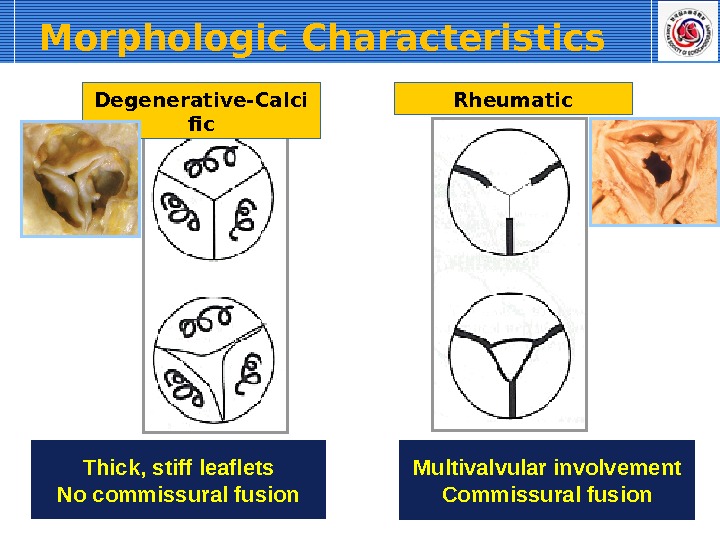
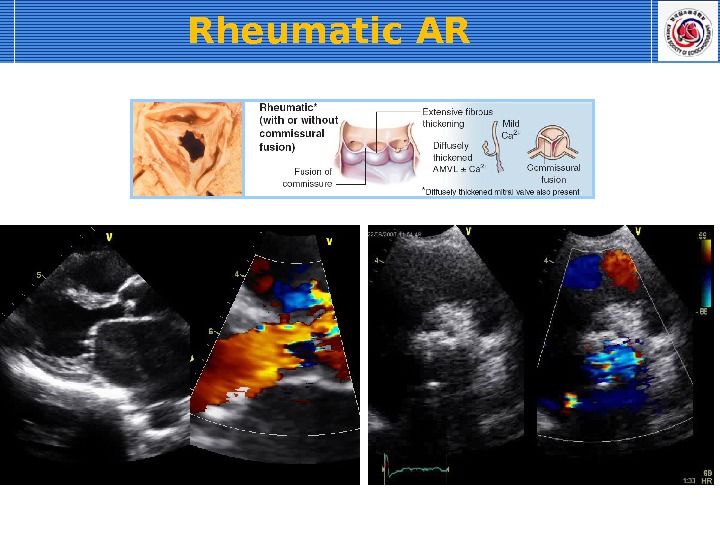
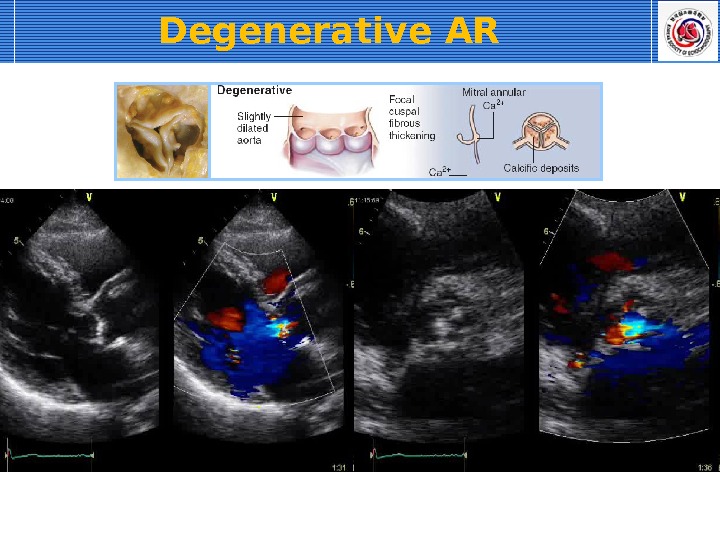
Morphologic Characteristics Degenerative-Calci fic Rheumatic Thick, stiff leaflets No commissural fusion Multivalvular involvement Commissural fusion
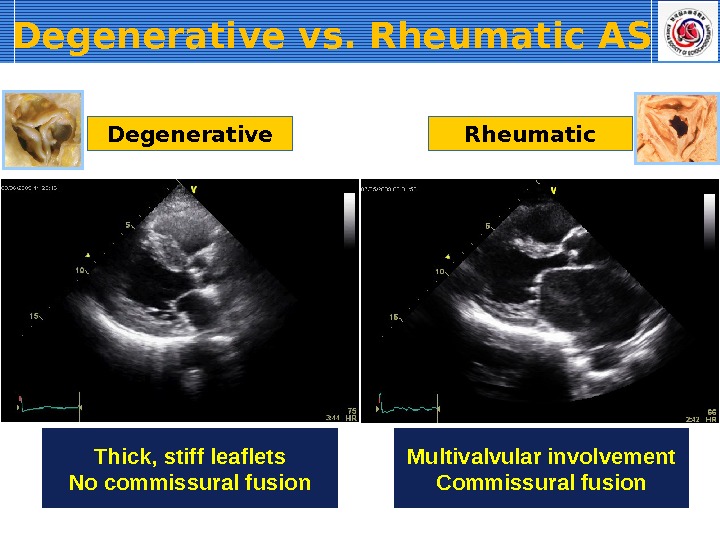
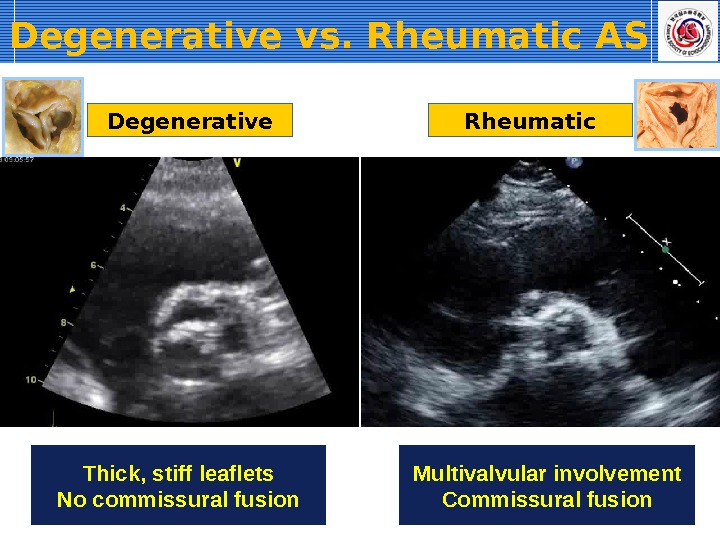
Degenerative vs. Rheumatic AS Thick, stiff leaflets No commissural fusion Degenerative Rheumatic Multivalvular involvement Commissural fusion
Thick, stiff leaflets No commissural fusion Multivalvular involvement Commissural fusion. Degenerative Rheumatic. Degenerative vs. Rheumatic AS
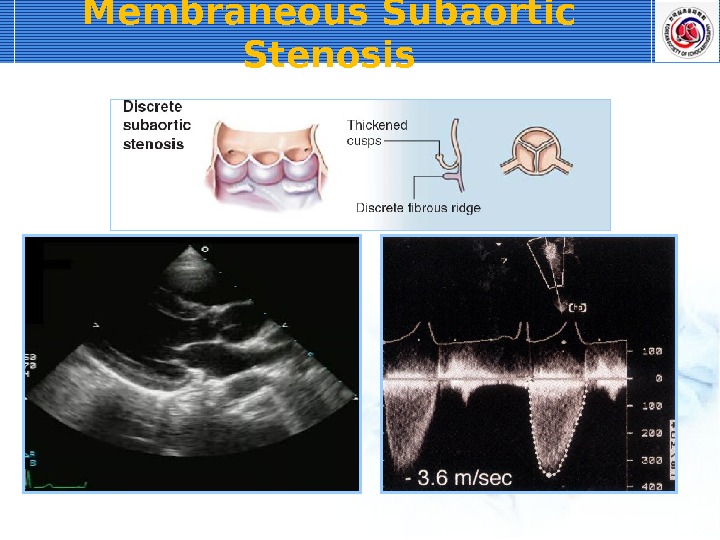
Membraneous Subaortic Stenosis
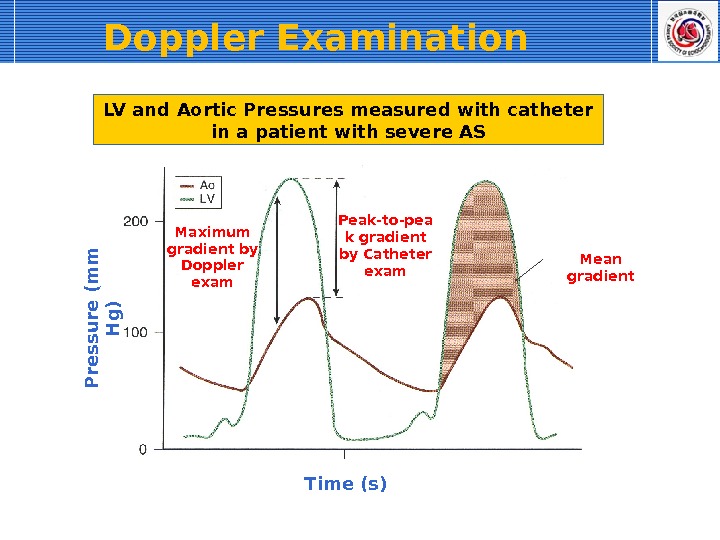
Doppler Examination Time (s)P re s s u re (m m H g )Maximum gradient by Doppler exam Peak-to-pea k gradient by Catheter exam Mean gradient. LV and Aortic Pressures measured with catheter in a patient with severe AS
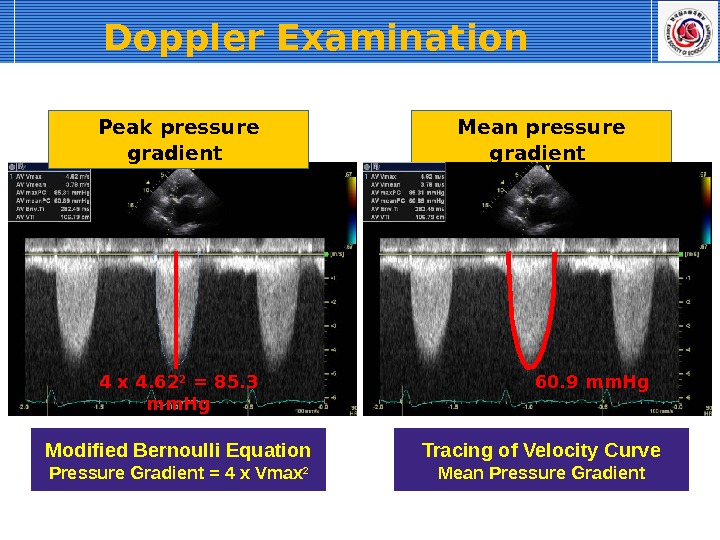
Peak pressure gradient Mean pressure gradient Modified Bernoulli Equation Pressure Gradient = 4 x Vmax 24 x 4. 62 2 = 85. 3 mm. Hg Tracing of Velocity Curve Mean Pressure Gradient 60. 9 mm. Hg. Doppler Examination
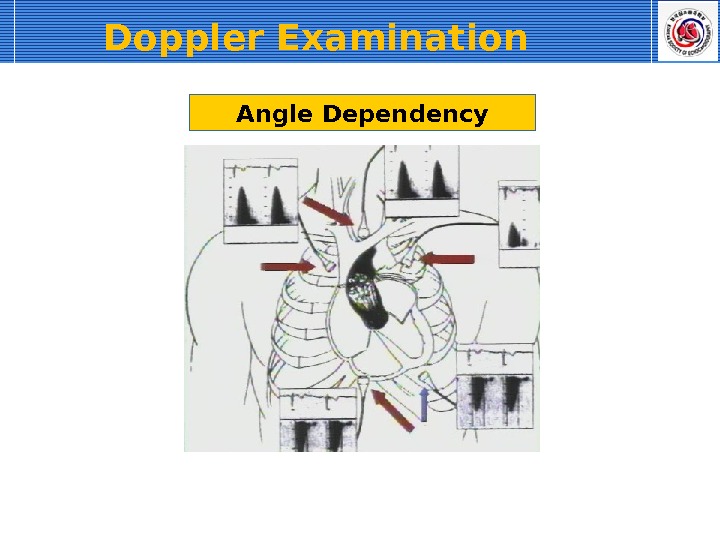
Angle Dependency. Doppler Examination
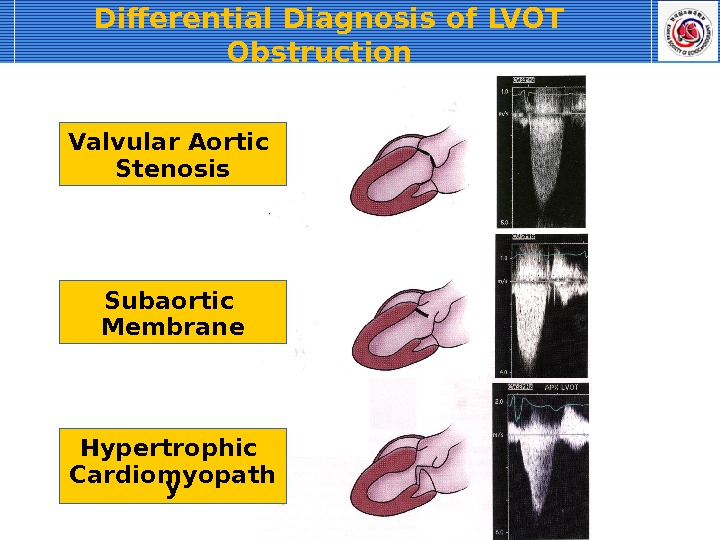
Differential Diagnosis of LVOT Obstruction Valvular Aortic Stenosis Subaortic Membrane Hypertrophic Cardiomyopath y
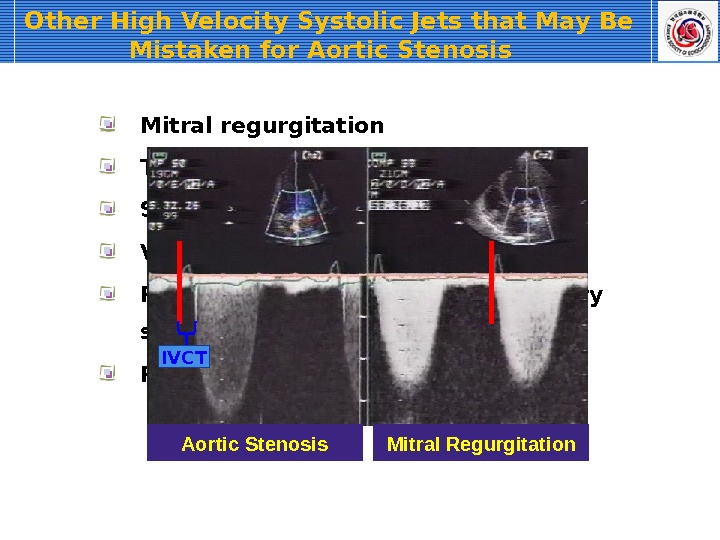
Other High Velocity Systolic Jets that May Be Mistaken for Aortic Stenosis Mitral regurgitation Tricuspid regurgitation Supravalvular stenosis Ventricular septal defect Pulmonic or branch pulmonary artery stenosis Peripheral vascular stenosis (e. q. , subclavian artery) IVCT Aortic Stenosis Mitral Regurgitation
Calculation of Valve Area 2 D Planimetry Continuity equation
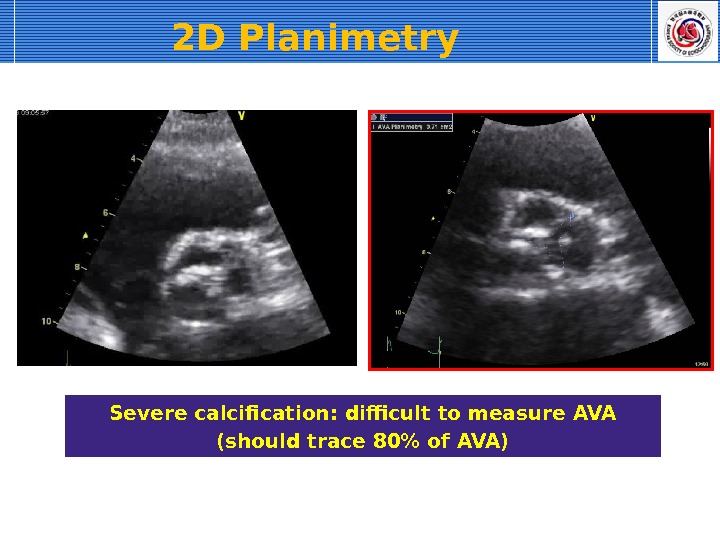
2 D Planimetry Severe calcification: difficult to measure AVA (should trace 80% of AVA)
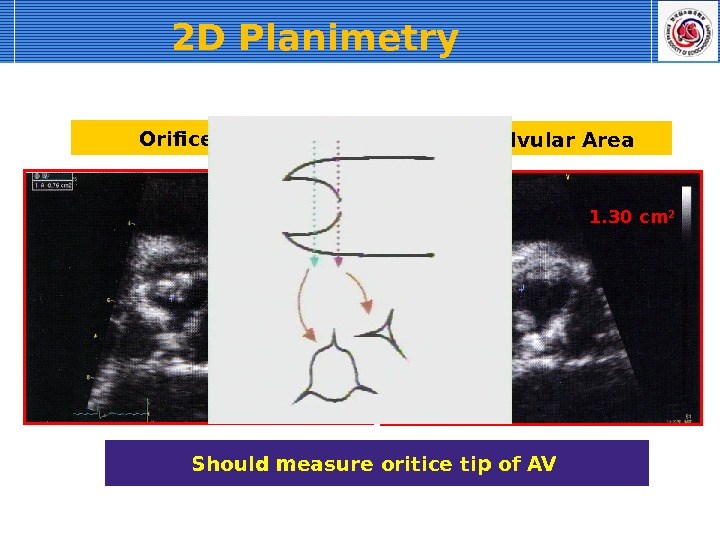
Should measure oritice tip of AV Subvalvular Area 1. 30 cm 2 Orifice Tip 0. 76 cm 22 D Planimetry
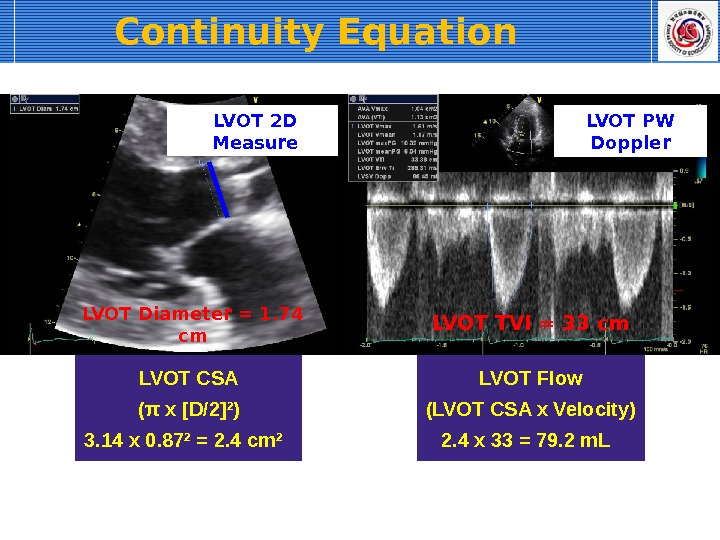
Continuity Equation LVOT Stroke Volume = AS-Jet Stroke Volume LVOT CSA x LVOT TVI = AVA x AS-Jet TVI AVA = (LVOT CSA x LVOT TVI) / AS-Jet TVI CSA LVO TTVI LVO T TVI AVCSA AVA = X
LVOT Diameter = 1. 74 cm LVOT CSA ( π x [D/2] 2 ) 3. 14 x 0. 87 2 = 2. 4 cm 2 LVOT 2 D Measure LVOT TVI = 33 cm LVOT Flow (LVOT CSA x Velocity) 2. 4 x 33 = 79. 2 m. L LVOT PW Doppler. Continuity Equation
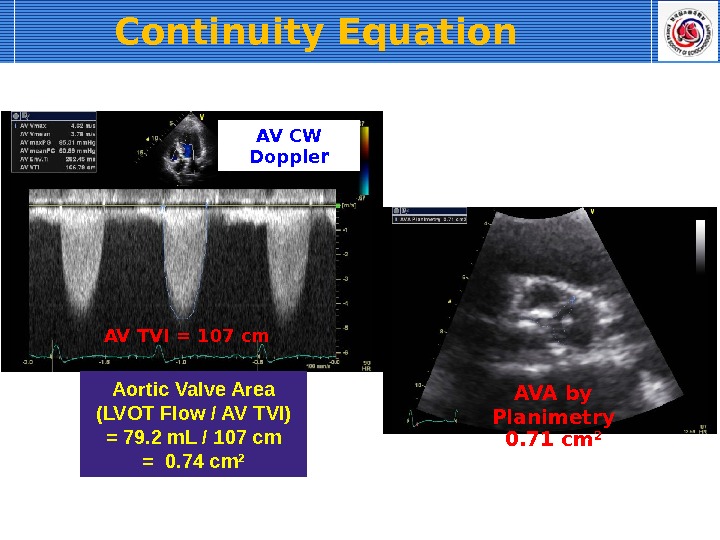
AV TVI = 107 cm Aortic Valve Area (LVOT Flow / AV TVI) = 79. 2 m. L / 107 cm = 0. 74 cm 2 AV CW Doppler AVA by Planimetry 0. 71 cm 2 Continuity Equation
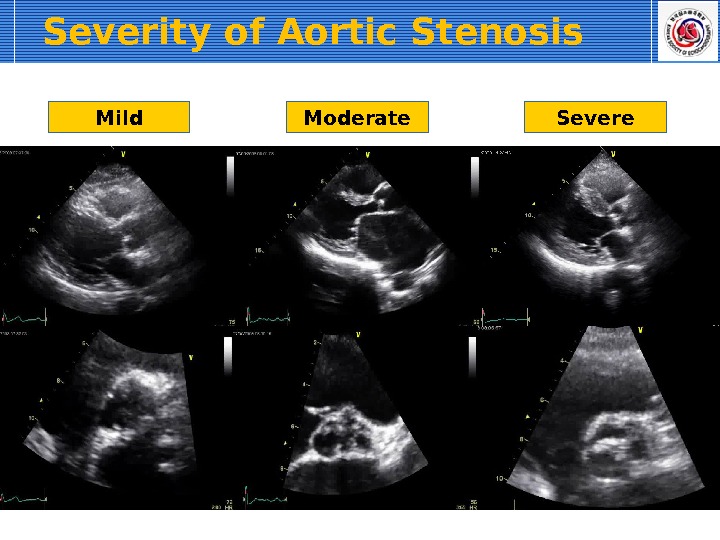
Severity of Aortic Stenosis Mild Moderate Severe
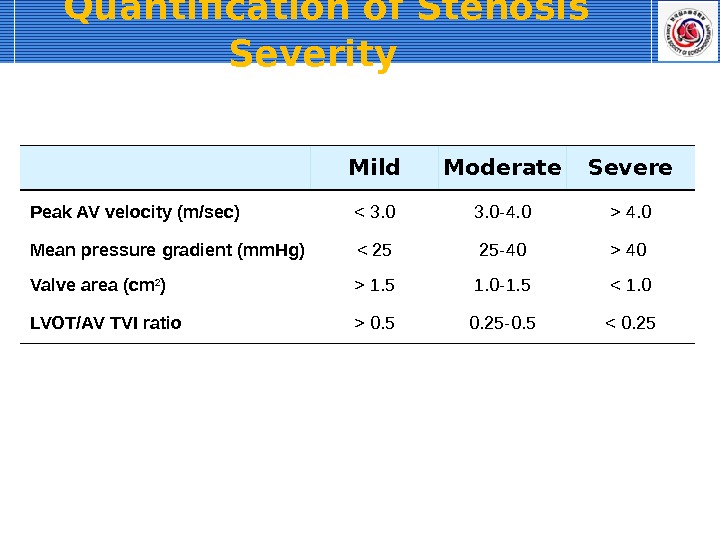
Quantification of Stenosis Severity Mild Moderate Severe Peak AV velocity (m/sec) 4. 0 Mean pressure gradient (mm. Hg) 40 Valve area (cm 2 ) > 1. 5 1. 0 -1. 5 0. 5 0. 25 -0. 5 < 0.
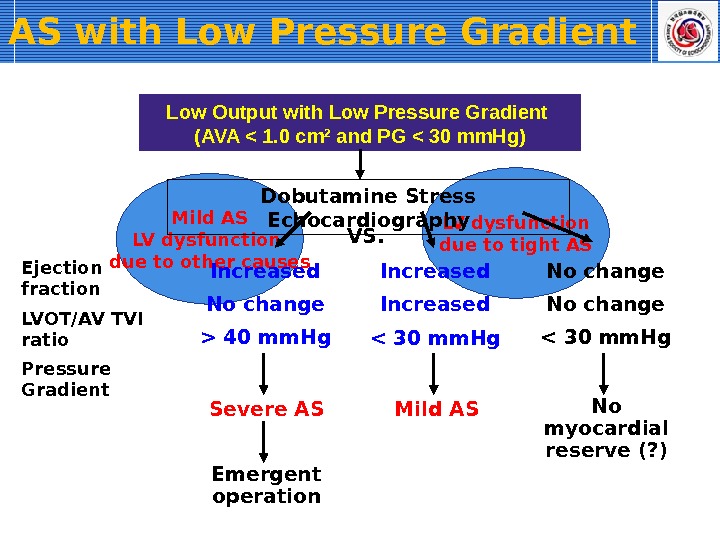
Mild AS LV dysfunction due to other causes LV dysfunction due to tight ASVS. AS with Low Pressure Gradient Low Output with Low Pressure Gradient (AVA < 1. 0 cm 2 and PG < 30 mm. Hg) Dobutamine Stress Echocardiography Ejection fraction LVOT/AV TVI ratio Pressure Gradient < 30 mm. Hg Increased Mild AS 40 mm. Hg No change Increased Severe AS Emergent operation
Aortic Regurgitation
Etiology of Aortic Regurgitation Cusp pathology Aortic wall pathology including aortitis Congenital
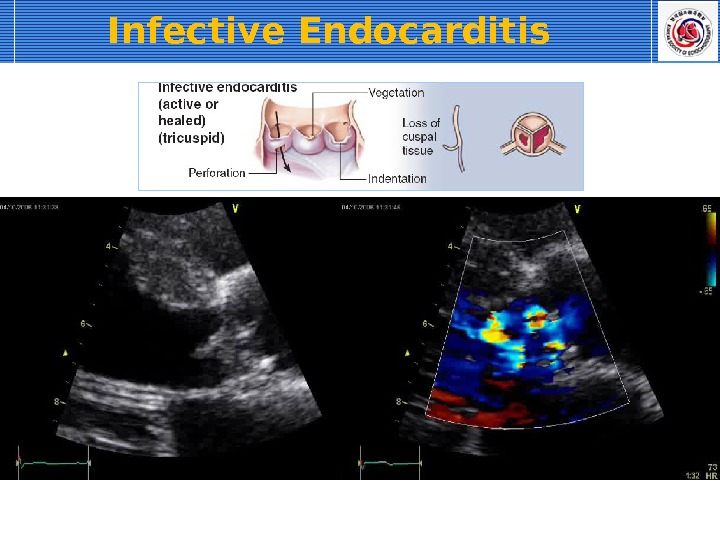
Cusp Pathology (Including congenital) Rheumatic Degenerative Infective endocarditis Congenitally bicuspid valve Ass. with membraneous subaortic stenosis Ass. with ventricular septal defect Aortic valve prolapse (Myxomatous or congenitally abnormal) Less common — Unicommissural and quadricuspid valve — Rupture of a fenestrated valve — SLE, RA, Ankylosing spondylitis, Takayasu disease, Whipple disease, Crohn disease etc
Rheumatic AR
Degenerative AR
Infective Endocarditis
Bicuspid Aortic Valve
Quadricuspid Aortic Valve
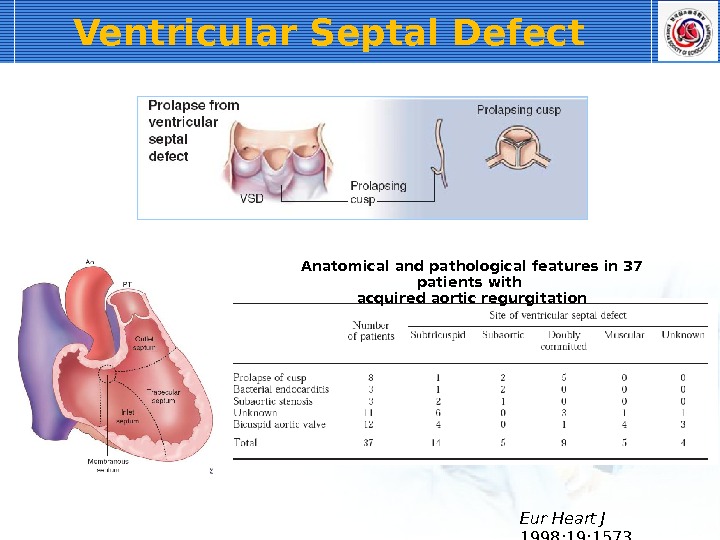
Ventricular Septal Defect Eur Heart J 1998; 19: 1573 Anatomical and pathological features in 37 patients with acquired aortic regurgitation
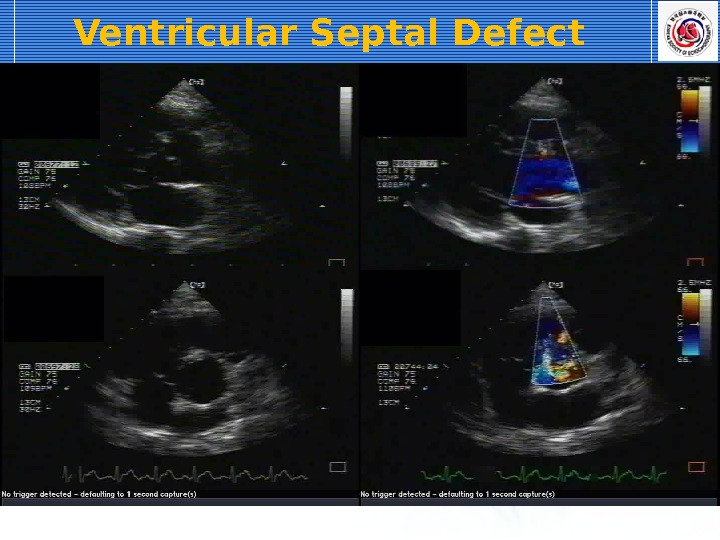
Ventricular Septal Defect
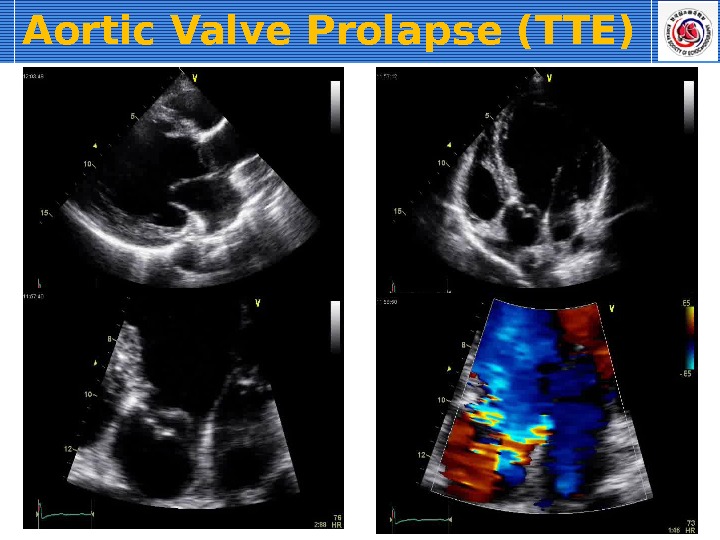
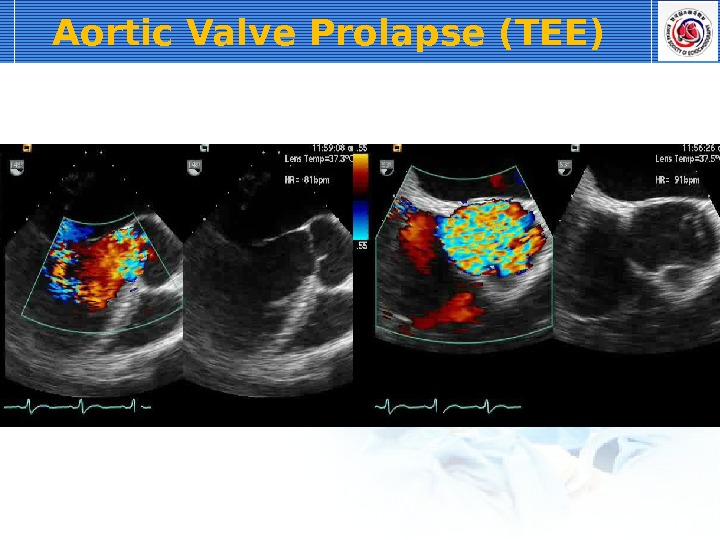
Aortic Valve Prolapse Best seen in parasternal long axis view Disruption of commissural support — Dissection — Dilatation — Ass. with VSD — Myxomatous or congenitally abnormality
Aortic Valve Prolapse (TTE)
Aortic Valve Prolapse (TEE)
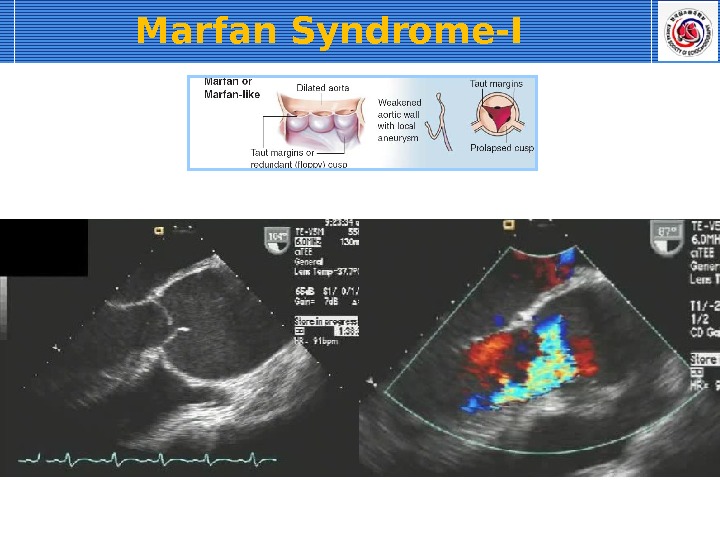
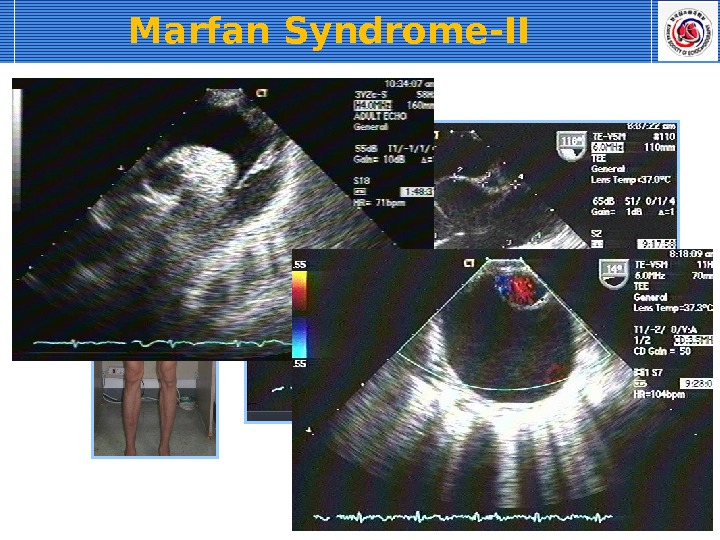
Aortic Root Disease Aortic dilatation related with — Hypertension — Age-related (degenerative) — Bicuspid AV Aortic dissection Cystic medial necrosis (Marfan syndrome) Takayasu arteritis Behcet’s disease Ankylosing spondylitis Less common — Syphilitic aortitis, psoriatic arthritis, UC, giant cell arteritis — relapsing polychondritis, Reiter syndrome
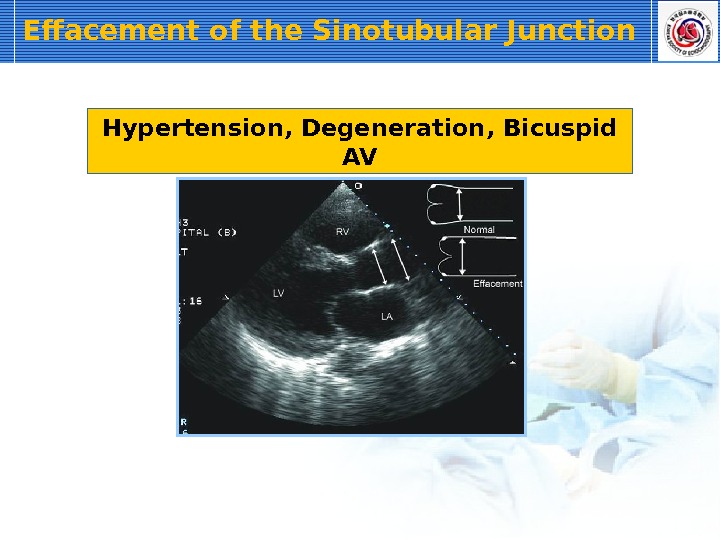
Effacement of the Sinotubular Junction Hypertension, Degeneration, Bicuspid AV
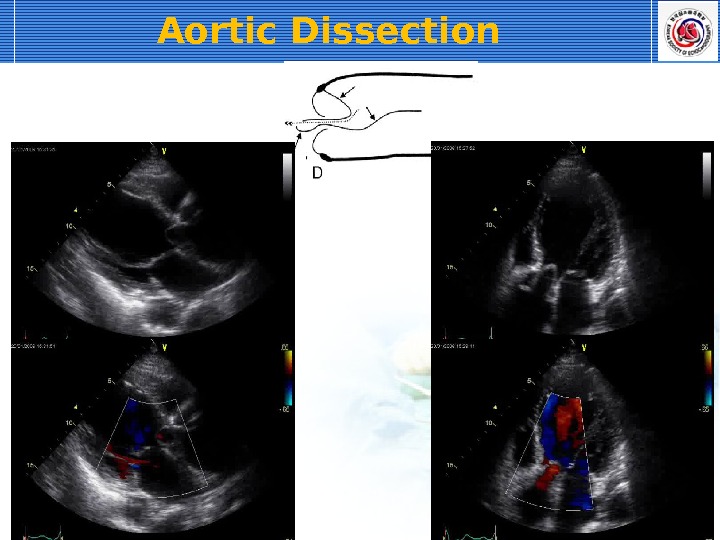
Aortic Dissection
Marfan Syndrome-I
Marfan Syndrome-II
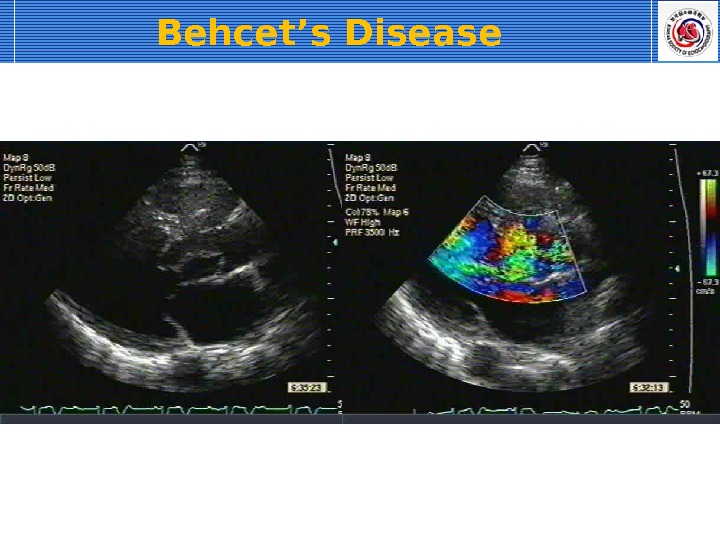
Behcet’s Disease
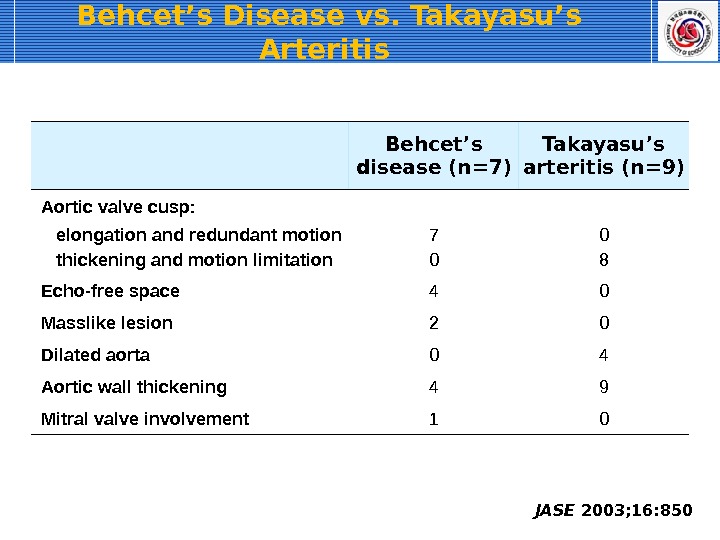
Behcet’s Disease vs. Takayasu’s Arteritis JASE 2003; 16: 850 Behcet’s disease (n=7) Takayasu’s arteritis (n=9) Aortic valve cusp: elongation and redundant motion 7 0 thickening and motion limitation 0 8 Echo-free space 4 0 Masslike lesion 2 0 Dilated aorta 0 4 Aortic wall thickening 4 9 Mitral valve involvement
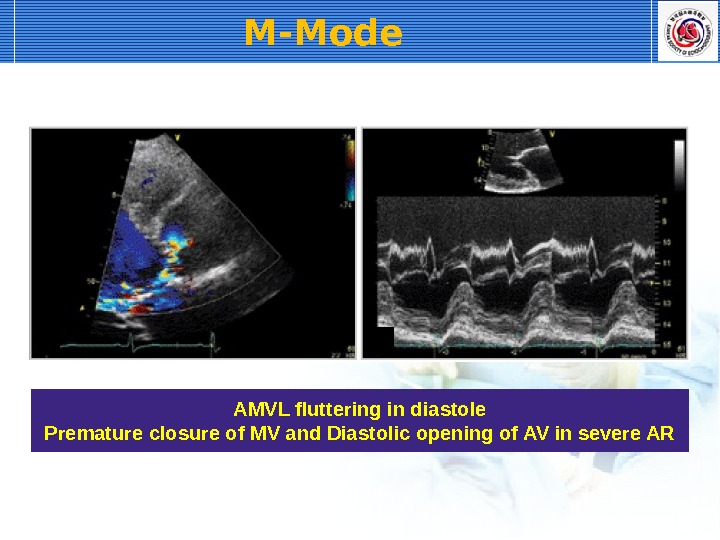
M-Mode AMVL fluttering in diastole Premature closure of MV and Diastolic opening of AV in severe AR
Estimating the Severity of AR Color Flow — Jet area/height — Vena contracta width — Flow convergence or PISA Continuous Wave Doppler — Signal density — Pressure half time (P ½ t) or Slope Pulsed Wave Doppler — Regurgitant volume/fraction — Descending aortic flow reversal 2 D Echocardiography — LV end-diastolic dimension — LV end-systolic dimension
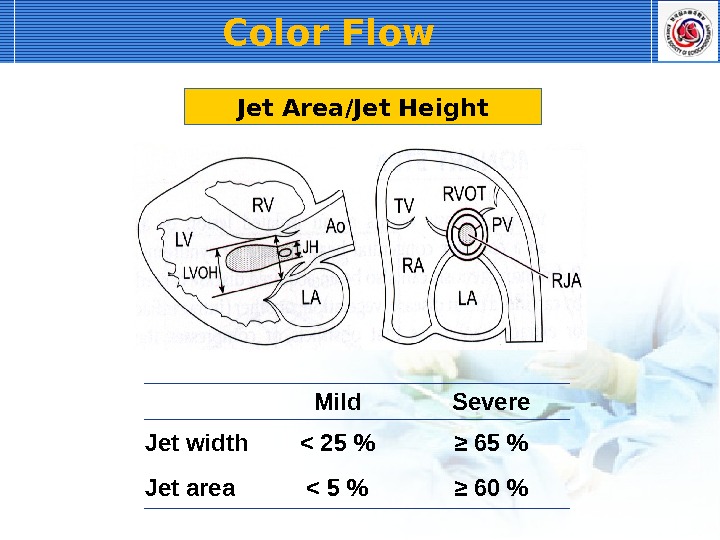
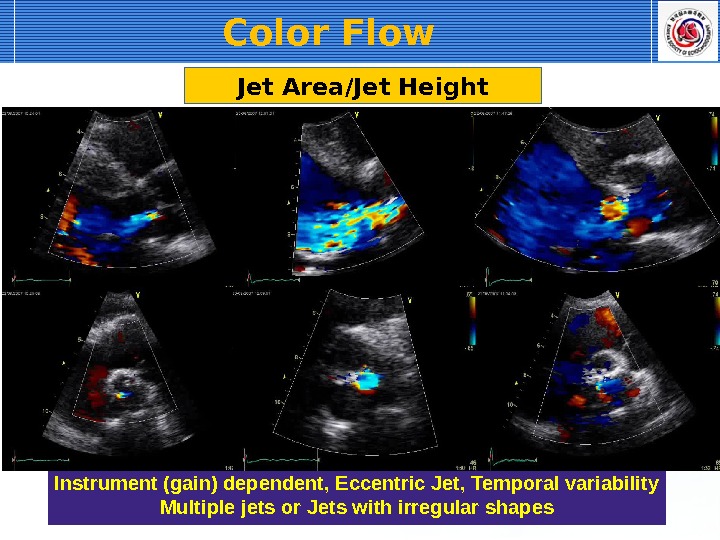
Color Flow Jet Area/Jet Height Mild Severe Jet width < 25 % ≥ 65 % Jet area < 5 % ≥ 60 %
Jet Area/Jet Height Instrument (gain) dependent, Eccentric Jet, Temporal variability Multiple jets or Jets with irregular shapes Color Flow
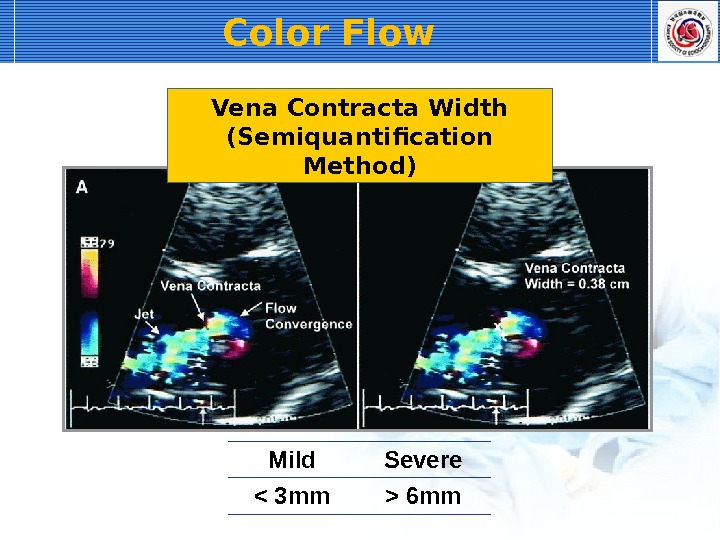
Vena Contracta Width (Semiquantification Method) Most narrow point : just below flow convergence reflect regurgitant orifice area Measure at zooming parasternal long axis view Vertical to AR jet : measure vena contracta width Color Flow
Mild Severe 6 mm. Vena Contracta Width (Semiquantification Method)Color Flow
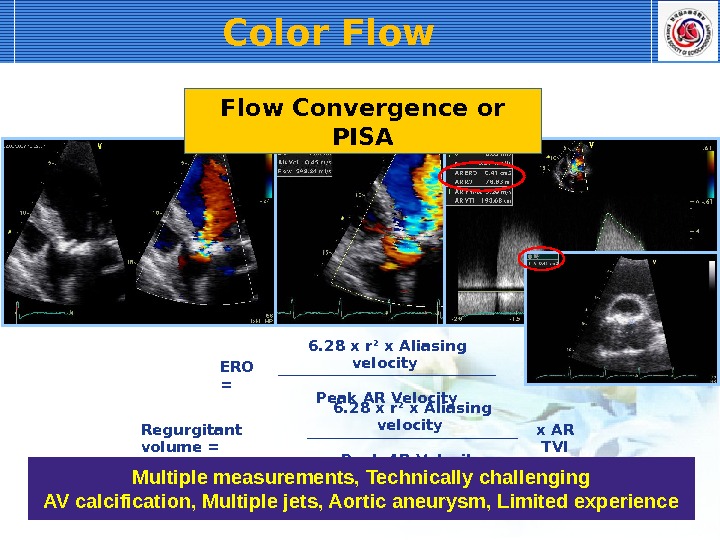
Color Flow ERO = 6. 28 x r 2 x Aliasing velocity Peak AR Velocity Regurgitant volume = 6. 28 x r 2 x Aliasing velocity x AR TVI Peak AR Velocity. Flow Convergence or PISA Multiple measurements, Technically challenging AV calcification, Multiple jets, Aortic aneurysm, Limited experience
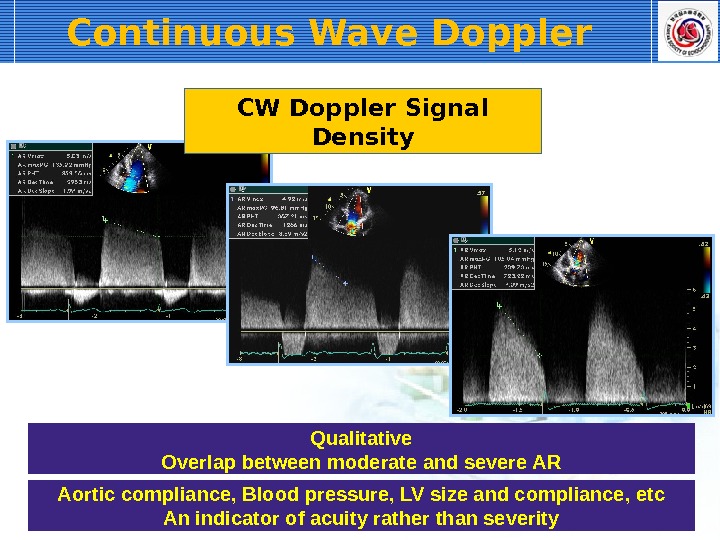
Continuous Wave Doppler CW Doppler Signal Density Qualitative Overlap between moderate and severe AR Aortic compliance, Blood pressure, LV size and compliance, etc An indicator of acuity rather than severity
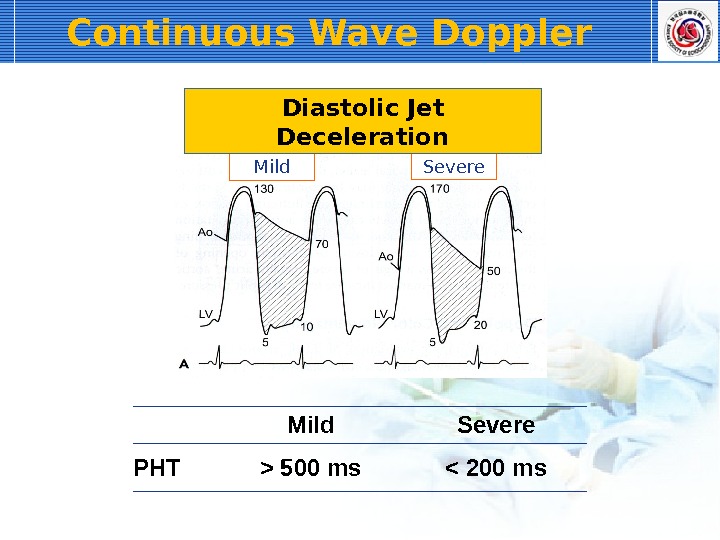
Continuous Wave Doppler Mild Severe PHT > 500 ms < 200 ms. Diastolic Jet Deceleration
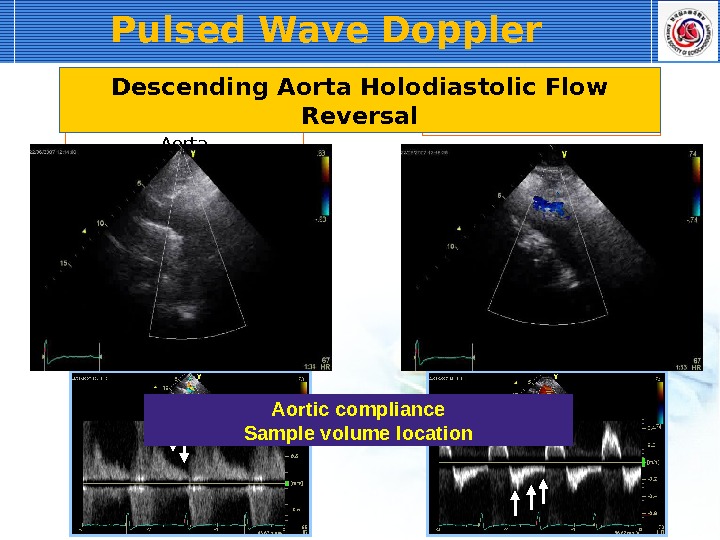
Pulsed Wave Doppler Descending Thoracic Aorta Abdominal Aorta. Descending Aorta Holodiastolic Flow Reversal Aortic compliance Sample volume location
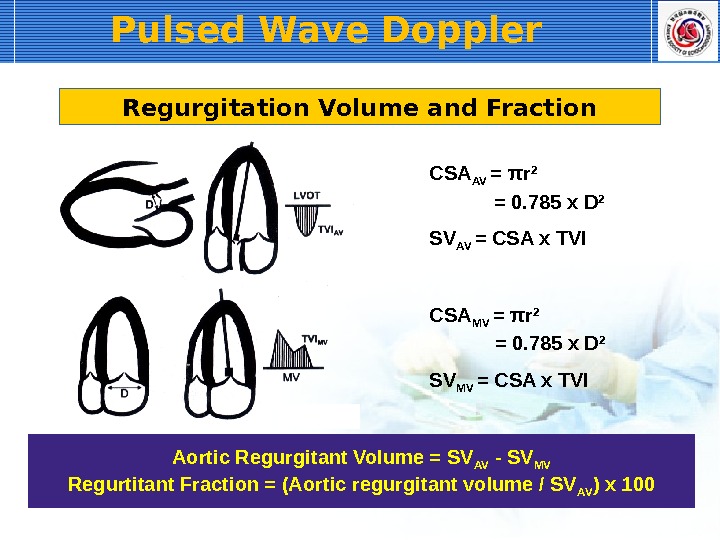
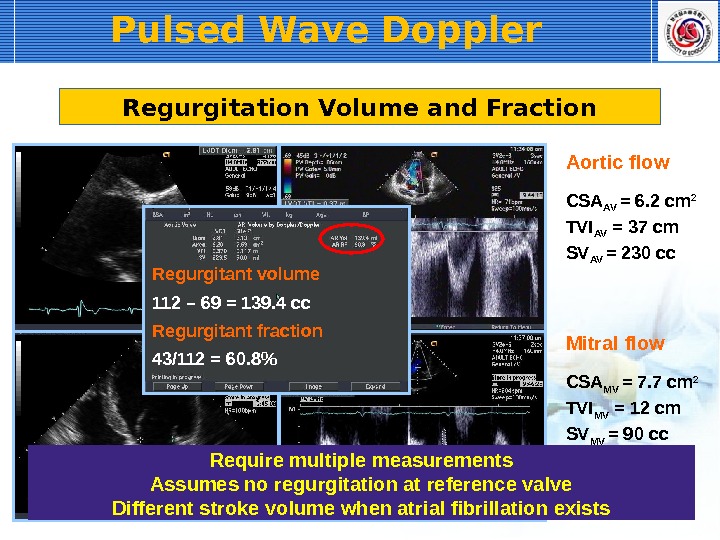
Pulsed Wave Doppler SV AV = CSA x TVICSA AV = π r 2 = 0. 785 x D 2 SV MV = CSA x TVICSA MV = π r 2 = 0. 785 x D 2 Regurgitation Volume and Fraction Aortic Regurgitant Volume = SV AV — SV MV Regurtitant Fraction = (Aortic regurgitant volume / SV AV ) x
Pulsed Wave Doppler CSA AV = 6. 2 cm 2 TVI AV = 37 cm SV AV = 230 cc. Aortic flow CSA MV = 7. 7 cm 2 TVI MV = 12 cm SV MV = 90 cc. Mitral flow. Regurgitation Volume and Fraction 112 – 69 = 139. 4 cc. Regurgitant volume 43/112 = 60. 8%Regurgitant fraction Require multiple measurements Assumes no regurgitation at reference valve Different stroke volume when atrial fibrillation exists
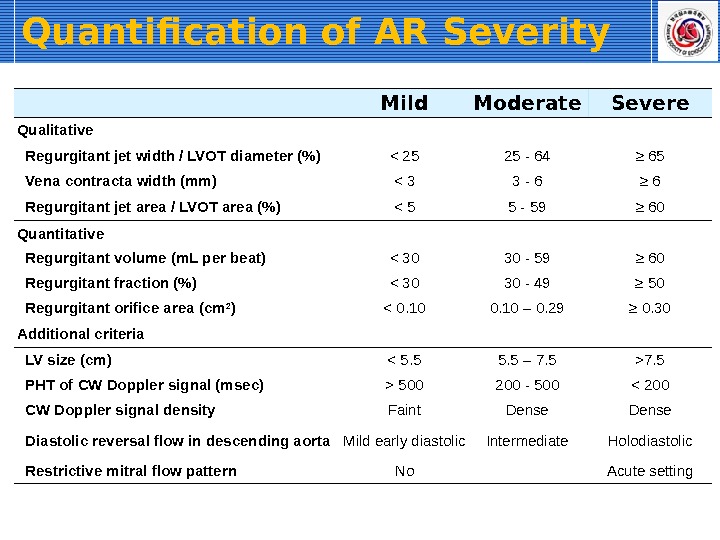
Quantification of AR Severity Mild Moderate Severe Qualitative Regurgitant jet width / LVOT diameter (%) < 25 25 — 64 ≥ 65 Vena contracta width (mm) < 3 3 — 6 ≥ 6 Regurgitant jet area / LVOT area (%) < 5 5 — 59 ≥ 60 Quantitative Regurgitant volume (m. L per beat) < 30 30 — 59 ≥ 60 Regurgitant fraction (%) < 30 30 — 49 ≥ 50 Regurgitant orifice area (cm 2 ) < 0. 10 – 0. 29 ≥ 0. 30 Additional criteria LV size (cm) 7. 5 PHT of CW Doppler signal (msec) > 500 200 — 500 < 200 CW Doppler signal density Faint Dense Diastolic reversal flow in descending aorta Mild early diastolic Intermediate Holodiastolic Restrictive mitral flow pattern No Acute setting
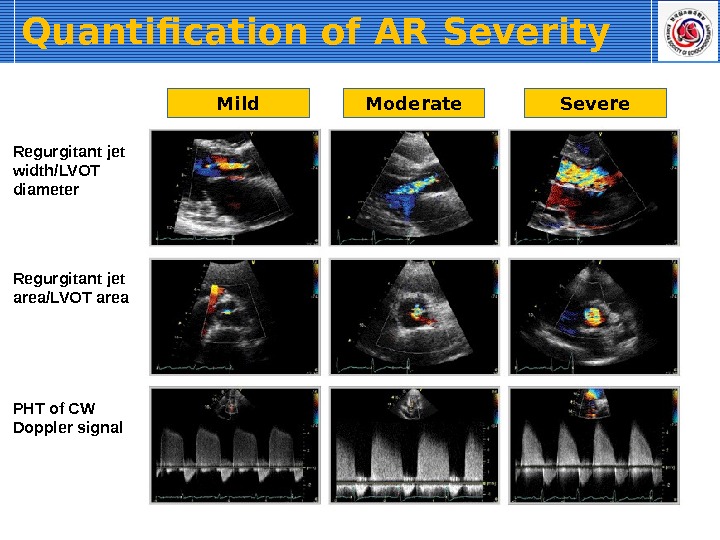
Mild Moderate Severe Regurgitant jet width/LVOT diameter Regurgitant jet area/LVOT area PHT of CW Doppler signal Quantification of AR Severity
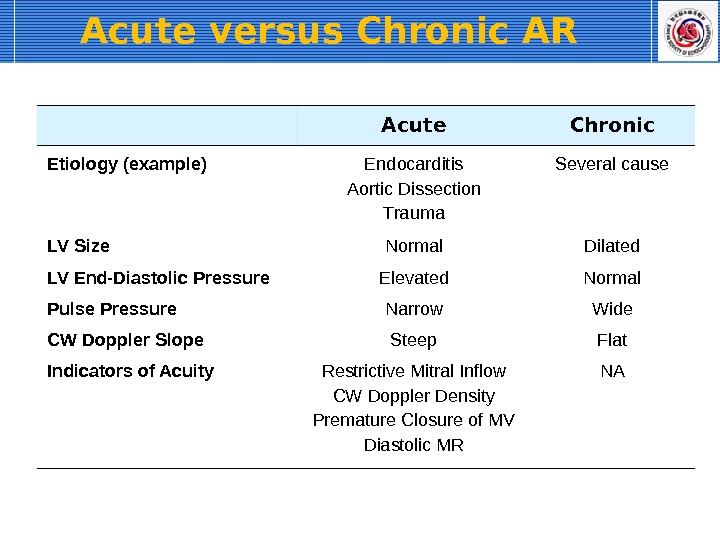
Acute versus Chronic AR Acute Chronic Etiology (example) Endocarditis Aortic Dissection Trauma Several cause LV Size Normal Dilated LV End-Diastolic Pressure Elevated Normal Pulse Pressure Narrow Wide CW Doppler Slope Steep Flat Indicators of Acuity Restrictive Mitral Inflow CW Doppler Density Premature Closure of MV Diastolic MR N
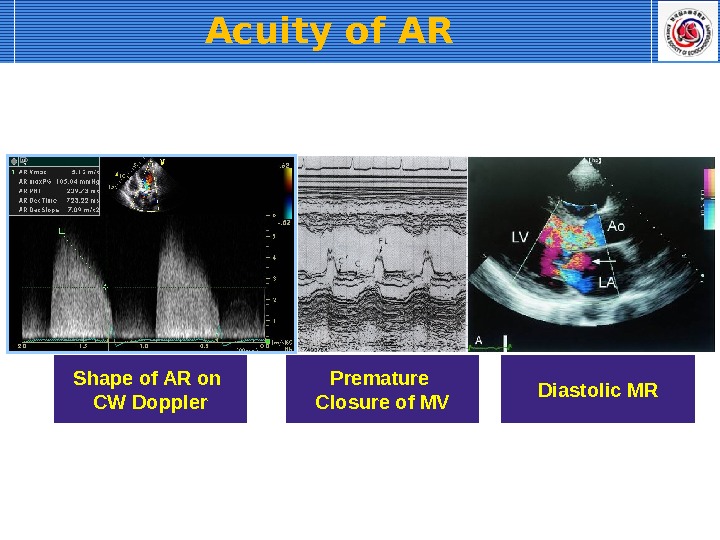
Acuity of AR Shape of AR on CW Doppler Premature Closure of MV Diastolic MR