8a09def238dd74149cc55f24cfb0b7ed.ppt
- Количество слайдов: 27



Anaesthesia Crisis Simulation

Background • Anaesthesia early adoption SBME • Driven by Gaba, Emily Bromily • Similarities commercial airlines • Increased monitor/environmental fidelity • EMAC courses

New Zealand • Both EMAC course providers in N Island • New anaesthetic registrar crisis course • More SBME for trainees near these centres But • Limited access for S island based Dr’s • Different equipment/environment • Lack of team based approach using local teams

Christchurch Anaesthetics • Limited SBME despite demand PROMPT EMAC Course x 1 in training CORE 7 EMST/APLS PATCH Ad hoc morning sessions

The Problem • SBME effective • Significant simulation debriefing resources • Dose response relationship • Fidelity important to a point – buy in • Full simulation suite facilities expensive and not realistic for peripheral centres
 Collaborative approach with Uo. OSC 2) Development novel approach")
Solutions • 2 avenues 1) Collaborative approach with Uo. OSC 2) Development novel approach using equipment already available in the hospital at no cost.

The “In situ” simulator • Clinical engineering calibration machines can be used to drive any monitor • This allows scenarios to be run “in situ” in the clinical environment

Sp 02

Sp 02 • “False finger” to attach Sp 02 probe • Dial up Sp 02 and HR • Realistically changes over a number of seconds • Sometimes a little temperamental • Short period of flat line when changes made

NIBP

NIBP • Useful graduations 60/40, 80/50, 100/60, 120/80 etc • Y connector!

MP 450 ECG, IBP

MP 450 ECG, IBP • Allows adjustment HR and common rhythms. • Also invasive BP trace but fixed at 120/80 so limited utility. • Must attach to 5 lead ECG for all rhythms to be available

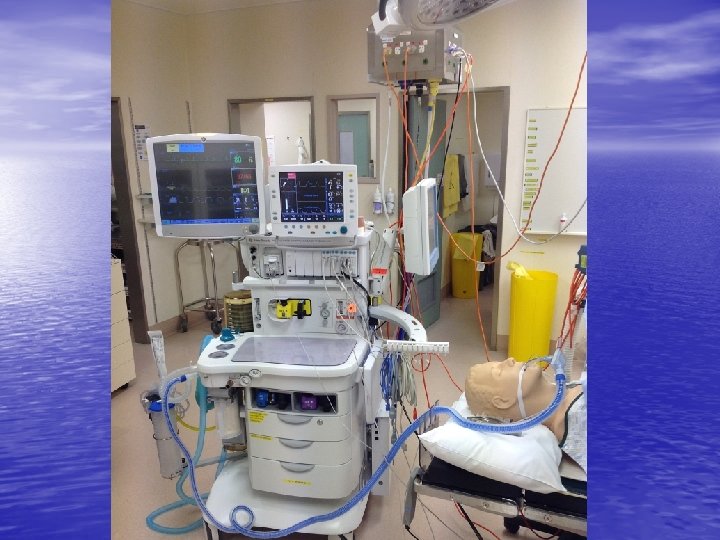
The In situ OT set up


Video

Junior Trainee Crisis Sessions • 0700 coffee, muffins, Non threatening • 4 scenarios (anaphylaxis, MI VF arrest in PACU, Aspiration on LMA, Blocked ETT) • 4 -6 trainees, 50% attended all. • Trainee tech • Guest “Volunteer” debriefer • Sign up sheet, evaluation survey and Post scenario resources provided on drop box

These scenarios have been a valuable learning experience

Fidelity

What were the strengths of the OT set up • More realistic, better prepared for real-life situation • Acting in real environment • same environment we spend the majority of our time in • • • which makes how we might respond to the situation in real life more realistic and how we make use of the resources in that environment. Familiar environment, with equipment that we use everyday. It's where we work and where we would actually experience these events Same environment as place of work. Realistic scenarios with added realism from use of usual monitors and anaesthetic machines.

Weaknesses of in OT set up • Already identified, but would be useful having people • • • playing their usual roles, ie real nurses Difficult to hear lung sounds, other people in scenario should have a card of what they can / cannot offer to do having a scenario where when you do call for help and you gets heaps of willing assistants who may not be the most skilled/appropriate to assist in that particular situation and the subsequent distraction/stress this can provide and/or strains on communication when having to deal with that and the emergency at hand. Acting outside usual roles is unrealistic but necessary. Within limitations of mannikin (aka can't actually have real patients having cardiac arrest. . . ) no real weaknesses Not using volatile is the only unrealistic aspect, but understandable.

Issues • Clinical area limited availability scrupulous control of equipment • Set up time/ chasing collecting bits • Potential for unskilled debrief vulnerable participants • Dropbox

Questions

8a09def238dd74149cc55f24cfb0b7ed.ppt