59061f0e6d2bb566bc5e23ab9b557762.ppt
- Количество слайдов: 47



ALZHEIMER’S DEMENTIA As I Understand it…. Bhagyashree Barlingay MD

PERSISTENCE OF MEMORY

Normal Ageing, MCI- mild cognitive impairment, Dementia.

Why Alzheimer’s Dementia? - 320 Million elderly people in India above the age of 65. - Prevalance of AD- 3. 7 million people - 1 in 1, 000 in age group 40 -65 years; - 1 in 5 over the age of 80 years. - Incidence Of AD – - Doubles every 10 years after the age of 60 years. - Cost of taking care of a dementia patient - Financial, social, mental, physical ! No cure yet!

COST OF DEMNTIA CARE

Focus of discussion 1. What is dementia? 2. What is the cause of dementia? 3. Can we prevent it? 4. Role of palliative and hospice care

समत भरश बदध

What is dementia? 1. Progressive loss of memory, language, orientation, judgment, visuospatial abilities. the commonest type is Alzheimer’s dementia (AD). The course of AD a prolonged goodbye!

AD Progression Progressive, irreversible brain disorder which is not a part of normal aging 1 Insidious onset of early symptoms often mistaken for age-related memory change 1 Disease progression leads to behavioral and cognitive changes 1 Variable disease progression and rate of decline 1 Risk factors: aging, family history 1, head injury 2 Healthy aging Amnestic MCI Clinically diagnosed A Amnestic MCI: AD brain memory changes may Cognitive problems; other decline start decades cognitive before accelerates functions OK; symptoms after AD brain show diagnosis compensates for changes Birth Normal age-related memory loss Total loss of independent function 40 60 Life Course MCI=mild cognitive impairment. 1. US Department of Health and Human Services. 2005 -2006 Progress Report on Alzheimer's Disease 2007. , 2. Van Den Heuvel C, et al. Prog Brain Res. 2007; 161: 303 -316. 80 Death

Progressive Decline in AD

Who used to live in this house? ---Cognition 1. Attention, 2. Memory, 3. Judgement, 4. Reasoning, 5. Language,

An Abandoned House

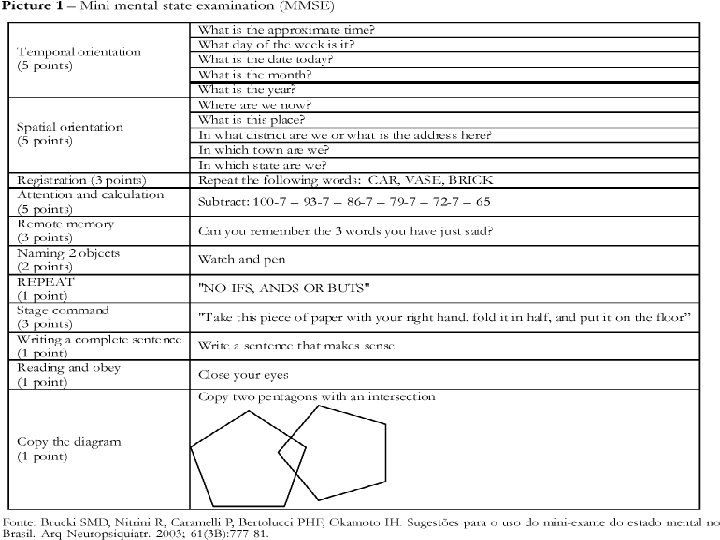
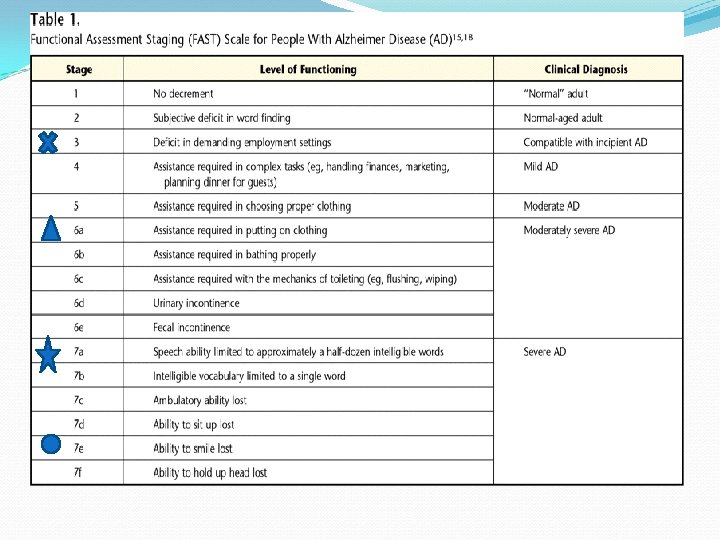
Assessment Scales MMSE – Dx, F/up, response to Rx. KFSS – placement in a facility FAST- used by hospice /medicare

KARNOFSKY PERFORMANCE STATUS SCALE 100 - Normal; no complaints; no evidence of disease. 90 - Able to carry on normal activity; minor signs or symptoms of disease. 80 - Normal activity with effort; some signs or symptoms of disease. 70 - Cares for self; unable to carry on normal activity or to do active work. 60 - Requires occasional assistance, but is able to care for most of his personal needs. 50 - Requires considerable assistance and frequent medical care. 40 - Disabled; requires special care and assistance. 30 - Severely disabled; hospital admission is indicated although death not imminent. 20 - Very sick; hospital admission necessary; active supportive treatment necessary. 10 - Moribund; fatal processes progressing rapidly. 0 - Dead

What are the risk factors for AD? Non-modifiable- Age, female gender, APOE genotype, family history. Modifiable- (mostly overlapping with Vascular dementia) Hypertension, type II DM, high cholesterol, metabolic syndrome, head injury, cerebrovascular disease, CKD, alcohol, depression, anemia. Inconclusive High homocysteine , dietary fat, estrogen, hearing loss, Vitamin D deficiency.

Brain healthy diet Veges- arugula, broccoli, brussels sprouts, boc choy, cabbage, cauliflower, kale, turnip, spinach, eggplant, corn, bell peppers. Fruits-berries, cherries, grapes, red grapes, oranges, plums, prunes. Fish- tuna salad – minimum mayo, halibut, grilled or smoked salmon, sardines. Drinks- green tea, pomegranate juice, red wine

Ha. Lad- curcumin Anti-inflammotory, Anti-cancer, Anti-amyloidogenic; But….

Alcohol 4 oz glass of table wine -14 gm of alcohol 12 oz bottle of american beer- 11. 5 gm of alcohol, 1. 5 oz of 80 -proof liquor in a mixed drink-18 gm of alcohol. 2 chemical- resveratrol and quercetin

What is metabolic syndrome? A cluster of risk factors for cardiovascular diseases including abdominal obesity, high triglycerides, low HDL, HTN, type II DM.

Why is Metabolic syndrome linked to AD? 1. High insulin levels are linked to cognitive decline. 2. Insulin degrading enzyme (IDE) helps take care of beta-amyloid as well along with insulin. 3. IDE levels are low in type II dm. 4. IDE has more affinity for insulin.

How does one decrease the risk of AD by acting on the modifiable risk factors? CHANGE YOUR LIFESTYLE….


What is Lifestyle? Lifestyle - social, mental, and physical activity - inversely associated with the risk for Alzheimer’s disease (AD). Midlife levels of cardio-respiratory fitness may predict risk of dementia later in life, independent of cerebrovascular disease.

Why would lifestyle modification affect the risk of Dementia? Three biologically plausible hypotheses have emerged – 1. The cognitive reserve hypothesis 2. The vascular hypothesis 3. The stress hypothesis

The cognitive reserve hypothesis suggests that mental activity, learning, and social interaction prevent or reduce cognitive deficits by activating brain plasticity and enhancing synaptogenesis and perhaps neurogenesis.

The vascular hypothesis suggests that social, mental, and physical activity prevents AD through reduction of cardiovascular disease and stroke.

The stress hypothesis suggests that active individuals have more positive emotional states and reduced stress.

Stress Down regulation of Hippocampal steroid receptors Dampening of negative feedback control of the adrenocortical axis resulting in high cortisol levels, hippocampal atrophy, and impaired cognition.

The storage of memory Medial Temporal Lobe

Role Of Education in AD Advanced Education >>> Higher cognitive reserve >>>Decreased impact of AD (not protection) Cognitive Activities in late life delay the onset of Dementia Normal Cognition premortem>>>on Autopsy , heavy AD pathology>>>but hypertrophic hippocampal neurons>>>higher language ability scores during life with advanced education.

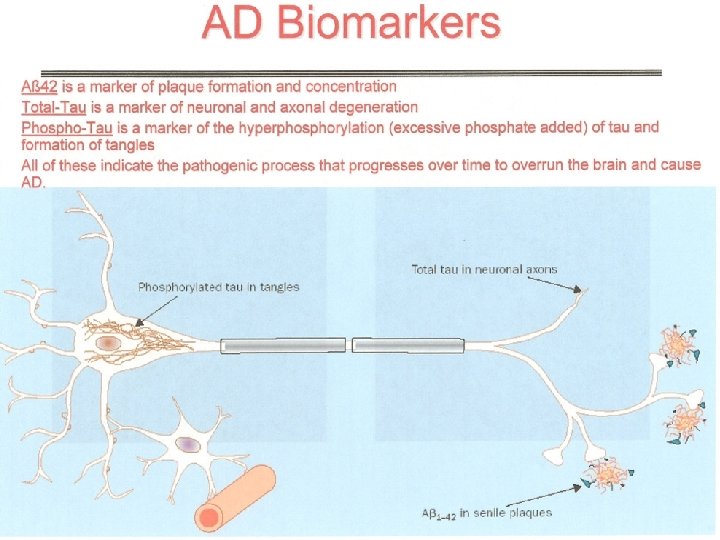
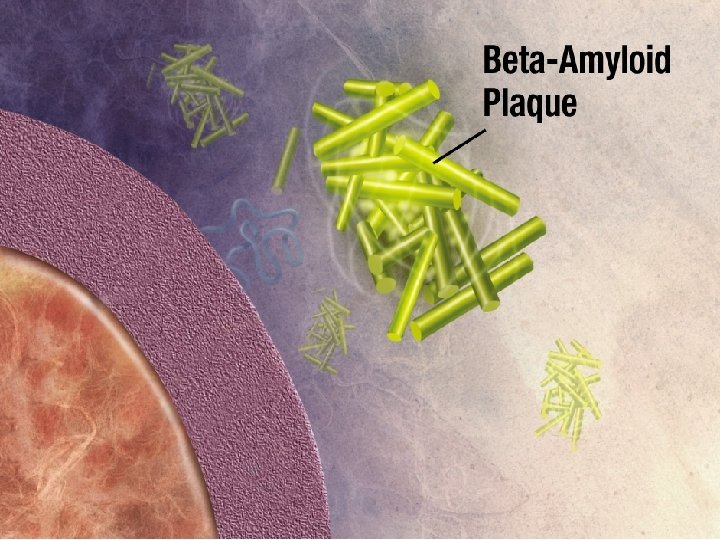
Pathology of AD Amyloid plaques Neurofibrillary tangles
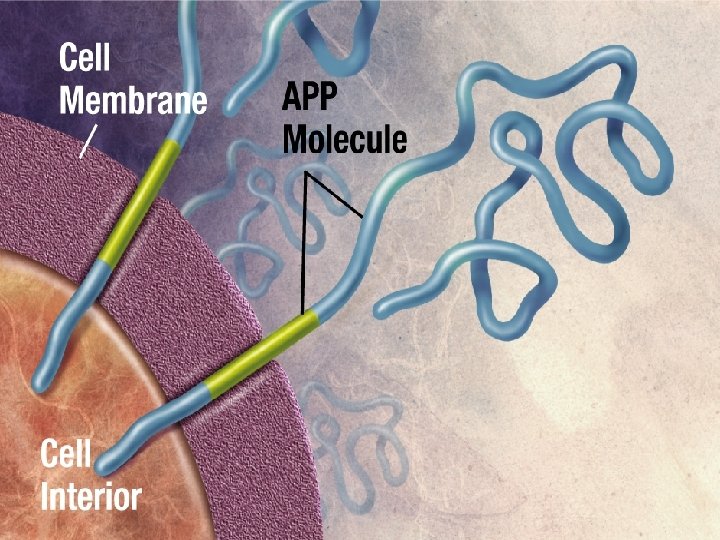

, Secretase Pathway: A Formation Amyloid plaque s. APP A secretase Oligomers secretase AICD • Cleavage is catalyzed by and secretases • The cleavage site is within the transmembrane 37

AD Progression Progressive, irreversible brain disorder which is not a part of normal aging 1 Insidious onset of early symptoms often mistaken for age-related memory change 1 Disease progression leads to behavioral and cognitive changes 1 Variable disease progression and rate of decline 1 Risk factors: aging, family history 1, head injury 2 Healthy aging Amnestic MCI Clinically diagnosed A Amnestic MCI: AD brain memory changes may Cognitive problems; other decline start decades cognitive before accelerates functions OK; symptoms after AD brain show diagnosis compensates for changes Birth Normal age-related memory loss Total loss of independent function 40 60 Life Course MCI=mild cognitive impairment. 1. US Department of Health and Human Services. 2005 -2006 Progress Report on Alzheimer's Disease 2007. , 2. Van Den Heuvel C, et al. Prog Brain Res. 2007; 161: 303 -316. 80 Death

Trajectory of Cancer Vs. . Dementia

END OF THE LIFE ISSUES COMPLICATIONS OF AD AGGRESSIVE TREATMENT AND CONSEQUENCES CARDIO-RESPIRATORY RESUSCITATION PROLONGATION OF LIFE EDUCATION OF THE FAMILY

To do list…. . 1 Make dementia a national priority 2 Increase funding for dementia research 3 Increase awareness about dementia 4 Improve dementia identification and care skills 5 Develop community support 6 Train caregivers 7 Develop comprehensive dementia care models 8 Develop new National Policies and Legislation, specially regarding end of the life issues. 9 Recommended books--

We are running out of time ---
59061f0e6d2bb566bc5e23ab9b557762.ppt