942fc595ea835fdd0d273a819513ae0f.ppt
- Количество слайдов: 93



AES 2010 Practice Management Course December 7, 2010 Gregory L. Barkley, M. D. Comprehensive Epilepsy Program Henry Ford Hospital Detroit, MI Associate Professor of Neurology Wayne State University

Outline Consultation Codes 2011 Medicare Conversion Factor and SGR October 2010 ICD-9 coding changes of interest 2011 CPT Codes PQRI update Gearing up for ICD-10 on October 1, 2013 Miscellaneous: Please note, I have removed the cell slice images from this set to keep the file size smaller. Images are at: http: //www. nytimes. com/slideshow/2010/11/29/science/20101130 -brain-1. html

Deadline extended until Dec 10. We specifically need members from: Alaska, Arizona, Arkansas Colorado, Connecticut Delaware, Kansas Kentucky, Maine Mississippi, Nebraska Nevada, North Dakota Rhode Island, South Carolina South Dakota, West Virginia Melissa Larson Manager, Advocacy Development AAN Professional Association Ph: 651. 695. 2748 FAX: 651. 361. 4848 mlarson@aan. com www. aan. comadvocacy

Consultation Codes Are Gone Forever • CMS stopped paying for consultations, 9924 x and 9925 x – In 2007, > 28 million claims – Money from Consultation codes redistributed to other physician codes to maintain budget neutrality • Other payers stopped paying for consults during 2010 • An attempt this year by AAN and other societies to get reconsideration of consult codes was rejected • CMS commented: "in most cases there is no substantial difference in physician work between E/M visits and services that would otherwise be reported with CPT consultation codes. "
 History Exam")
Coding an outpatient New Patient visit (3/3 or Hx, PE, and MDM) History Exam Decision Time Code elements making (minutes) HPI 1 -3 facts 1 -5 Straightforward 10 99201 HPI 1 -3 facts ROS 1 fact 6 Straightforward 20 99202 HPI 4 facts ROS 2, PSFH 1 12 low 30 99203 HPI 4 facts, ROS 10, PSFH 3 25 moderate 45 99204
 History Exam")
Coding an outpatient Established Patient visit (2/3 MDM + Hx or PE) History Exam elements Decision making Time (minutes) Code - - Minimal or none 5 99211 HPI 1 -3 facts 1 -5 Straightforward 10 99212 HPI 1 -3 facts ROS 1 6 low 15 99213 HPI 4 facts, ROS 2, PSFH 1 12 moderate 25 99214 HPI 4 facts, ROS 10, PSFH 3 25 high 40 99215
 History (CC always needed) Exam")
9922 x Coding an inpatient Initial Care Day (3/3) History (CC always needed) Exam elements Decision making Time Code (w. RVU) HPI 4 facts, 1 PFSH, 2 -9 ROS 12 Neuro SSE or 5 -7 systems Straight-forward or low 30 99221 (1. 89) HPI 4 facts, 3 PFSH, 10 ROS Full Neuro SSE (25) or 8 Systems Moderate (2 Chronic with 1 exacerbation) 50 99222 (2. 57) HPI 4 facts, Full Neuro High 70 99223 (minutes)
 History Exam Decision making Time")
9923 x Coding an inpatient Subsequent Day Care (2/3) History Exam Decision making Time Code (w. RVU) HPI 1 -3 facts 1 -5 straight-forward or low 15 99231 (0. 76) HPI 1 -3 facts ROS 1 fact 6 moderate 25 99232 (1. 39) HPI 4 facts ROS 2 facts 12 high 35 99233 (2. 00) elements (minutes)

Counseling and Coordination of Care Counseling is a discussion with patient or family about diagnoses, test results, recommended tests, prognosis, treatment alternatives, compliance, risk factor reduction, and patient and family education. Coordination of care is arranging for care with other health care providers. This includes any type of such activity.

Counseling and Coordination of Care • • • This can be used in place of the above HX-PE-MDM. It uses time to set LOS The documentation should state: – Minutes spent face-to-face – – • That more than 50% of time was counseling and/or coordinating care, Give some general idea of what counsel/coord. care. Time is: – Face-to-face with patient (outpatient) – • At bedside and on unit/floor (inpatient). No history or exam elements are needed except, of course, for real patient care purposes!

Emergency Room Care • • • Most ER services provided by neurologists and neurosurgeons are as “consultants” Use Established Patient (99211 -99215) codes for Medicare patients seen by anyone in your group in the past three years Otherwise use Outpatient New Patient (99201 -99205) codes If the patient is admitted to the hospital, then use the initial hospital day codes (99221 -99223) Critical Care services provided in ER, e. g. t. PA or status epilepticus management: – Use Critical Care codes 99291 - 99292
")
Critical Care • • • 99291 first hour of critical care (31 -74 minutes) 99292 each additional 30 minutes Coded by time for bedside and unit physician work for an unstable, critically ill patient – Not for consultant's time – Need not be continuous in any location • Generally cannot bill other E/M on same day. • Exceptions are if an E & M is performed at one time, then a crisis occurs and critical services are performed. • Make sure you document times carefully so you do not appear to be combining times of routine care with critical care times or procedure times. • Not every day in the ICU is critical care!!! – Patients awaiting transfer to GPU are not critically ill • Critical care can be provided anywhere including in the clinic • You must document time spent and what you did in your note

A Very Short Primer on American Health Care Financing: $2. 5 trillion spent on health care in 2009. Private insurance covered 59% of Americans. Government programs paid for 53% of direct health care costs and 62% if tax exemptions counted. More than 50 million Americans without health care coverage. Private insurance policies - Largely paid for by employers - Usually small, but increasing, out-of-pocket costs borne by individuals - Thousands of companies offering tens of thousands of individual policies - Range minimal coverage for catastrophic illness to full coverage Medicare Trust Fund - Elderly and those qualifying for Medicare disability -For outpatient care, covers 80% of professional fee schedule for visits and procedures + APC for technical charges - In 2006 outpatient medications were covered - For inpatient care, covers 80% of fee schedule for professional costs + DRG for technical costs - Covers 55% of psychiatric care charges (Chapter 5 of ICD-9)

In 2007, U. S per capita health care spending was $7, 290, 2. 5 times the OECD average and 16% of GDP U. S. government alone already pays more than total costs in nearly all other countries
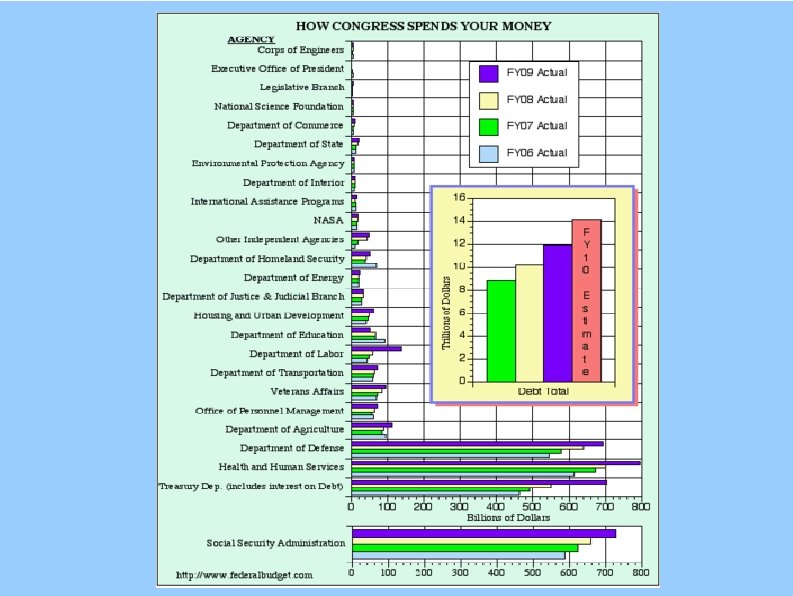

Health Care Spending is 16% of GDP

To Control US Debt Only options are to: Cut Medicare spending 2010 Accountable Care Act reduces Medicare spending by $350 Billion over 10 years Cut Social Security spending Cut Defense spending Raise taxes Reality is that all of the above are necessary

Social Security P. Krugman, NYTimes 12/06/2010

2011 Medicare Proposed Conversion Rate issued 11/02/2010, 2023 pages In the final rule, the Medicare Conversion Factor will be $25. 5217 starting 01/01/2011 – 30% drop compared to 2010 to meet SGR law – Conversion factor law override from 06/01/2010 until 11/30/2010 was $36. 8729 – Comment period is open until January 3, 2011 A 2. 2% increase from 2009 and averted a 21. 5% cut Legislation proposals in Congress to override remain contentious at this time – – On 11/18/2010, Senate passed a one month extension of current pay scale House passed same bill on 11/30/2010 Rescaling of RVU weights (-8. 2%) and (+0. 5%) budget neutrality change due to RVU changes mandated by law, so CF likely to be $34. 00 if Congress overrides

2011 Medicare Conversion Rate 12/06/2010, 8: 17 PM To: mem@lyris. aan. com From: mamery@aan. com Re: SGR Agreement Dear MEM Members: The Senate Finance committee just announced a one year delay of the SGR cuts. The deal will be fully paid for. Details to come. Michael J. Amery, Esq. Legislative Counsel American Academy of Neurology 202 -506 -7468

SGR Annual Override. . • Does not fixed flawed formula and increases the decrease needed the next year, currently $210 -279 B AMA

2011 ICD-9 Code Changes On October 1 of each year, the ICD-9 code changes occur There are new codes as well as new index terms. – Index terms can be used by coders to map to a specific code New index terms for epilepsy I presented at the ICD Coding and Maintenance Committee Meeting on 9/25/2008, my presentation is at: http: //www. cdc. gov/nchs/icd 9 cm_maintenance. htm Epilepsy, epileptic (idiopathic) 345. 9 Note: use the following fifth-digit subclassifications with categories 345. 0, 345. 1, 345. 4 -345. 9 0 1 without mention of intractable epilepsy with intractable epilepsy pharmacoresistant (pharmacologically resistant) poorly controlled refractory (medically) treatment resistant

2011 ICD-9 Code Changes 345 Epilepsy and recurrent seizures 780 General symptoms Delete Excludes: progressive myoclonic epilepsy (333. 2) 780. 3 Convulsions New code 780. 33 Post traumatic seizures Excludes: post traumatic epilepsy (345. 00 -345. 91)

2011 ICD-9 Code Changes 225 Benign neoplasm of brain and other parts of nervous system Revise Excludes: neurofibromatosis (237. 70 -237. 79) 237 Neoplasm of uncertain behavior of endocrine glands and nervous system 237. 7 Neurofibromatosis Delete von Recklinghausen's disease New code 237. 73 Schwannomatosis New code 237. 79 Other neurofibromatosis

2011 ICD-9 Code Changes Codes in Red are in Chapter 5, reimbursed at 55% vs. 80% 278. 0 Overweight and obesity New code 278. 03 Obesity hypoventilation syndrome Pickwickian syndrome 307 Special symptoms or syndromes, not elsewhere classified Revise 307. 0 Stuttering Adult onset fluency disorder Add Excludes: childhood onset fluency disorder (315. 35) Revise stuttering (fluency disorder) due to late effect of cerebrovascular accident (438. 14) Add fluency disorder in conditions classified elsewhere (784. 52)

2011 ICD-9 Code Changes Codes in Red are in Chapter 5, reimbursed at 55% vs. 80% 315 Specific delays in development 315. 3 Developmental speech or language disorder New code 315. 35 Childhood onset fluency disorder Cluttering NOS Stuttering NOS Excludes: adult onset fluency disorder (307. 0) fluency disorder due to late effect of cerebrovascular accident (438. 14) fluency disorder in conditions classified elsewhere (784. 52) 315. 39 Other Delete Excludes: stammering and stuttering (307. 0)

2011 ICD-9 Code Changes 337 Disorders of the autonomic nervous system Revise Use additional code to identify the cause, such as: fecal impaction (560. 32) 488 Influenza due to certain identified influenza viruses 337. 3 Autonomic dysreflexia 488. 0 Influenza due to identified avian influenza virus New code 488. 09 Influenza due to identified avian influenza virus with other manifestations Avian influenza with involvement of gastrointestinal tract Encephalopathy due to identified avian influenza Excludes: "intestinal flu" [viral gastroenteritis] (008. 8)

2011 ICD-9 Code Changes 488. 1 Influenza due to identified novel H 1 N 1 influenza virus New code 488. 19 Influenza due to identified novel H 1 N 1 influenza virus with other manifestations Encephalopathy due to identified novel H 1 N 1 influenza Novel H 1 N 1 influenza with involvement of gastrointestinal tract Excludes: "intestinal flu" [viral gastroenteritis] (008. 8) 721 Spondylosis and allied disorders 721. 4 Thoracic or lumbar spondylosis with myelopathy 721. 42 Lumbar region Delete Spondylogenic compression of lumbar spinal cord

2011 ICD-9 Code Changes 724 Other and unspecified disorders of back 724. 0 Spinal stenosis, other than cervical Revise 724. 02 Lumbar region, without neurogenic claudication Add Lumbar region NOS New code 724. 03 Lumbar region, with neurogenic claudication 742 Other congenital anomalies of nervous system 742. 8 Other specified anomalies of nervous system Revise Excludes: neurofibromatosis (237. 70 -237. 79)

2011 ICD-9 Code Changes 781 Symptoms involving nervous and musculoskeletal systems Revise 781. 8 Neurologic neglect syndrome Add Excludes: visuospatial deficit (799. 53) New code V 13. 63 Personal history of (corrected) congenital malformations of nervous system V 49 Other conditions influencing health status V 49. 8 Other specified conditions influencing health status New code V 49. 86 Do not resuscitate status

2011 ICD-9 Code Changes 784 Symptoms involving head and neck 784. 5 Other speech disturbance Revise Excludes: stammering and stuttering (315. 35) Delete that of nonorganic origin (307. 0, 307. 9) New code 784. 52 Fluency disorder in conditions classified elsewhere Stuttering in conditions classified elsewhere Code first underlying disease or condition, such as: Parkinson’s disease (332. 0) Excludes: adult onset fluency disorder (307. 0) childhood onset fluency disorder (315. 35) fluency disorder due to late effect of cerebrovascular accident (438. 14)

2011 ICD-9 Code Changes 799 Other ill-defined and unknown causes of morbidity and mortality New Subcategory 799. 5 Signs and symptoms involving cognition Excludes: amnesia (780. 93) amnestic syndrome (294. 0) attention deficit disorder (314. 00 -314. 01) late effects of cerebrovascular disease (438) memory loss (780. 93) mild cognitive impairment, so stated (331. 83) specific problems in developmental delay (315. 00 -315. 9) transient global amnesia (437. 7) visuospatial neglect 781. 8

2011 ICD-9 Code Changes 799 Other ill-defined and unknown causes of morbidity and mortality New code 799. 51 Attention or concentration deficit New code 799. 52 Cognitive communication deficit New code 799. 53 Visuospatial deficit New code 799. 54 Psychomotor deficit New code 799. 55 Frontal lobe and executive function deficit New code 799. 59 Other signs and symptoms involving cognition

2011 ICD-9 Code Changes 992 Effects of heat and light 992. 0 Heat stroke and sunstroke Add Use additional code(s) to identify any associated complication of heat stroke, such as: Add alterations of consciousness (780. 01 -780. 09) Add systemic inflammatory response syndrome (995. 93 -995. 94)
 Changes • Second year of 4 year transition on PE")
2011 Practice Expense (PE) Changes • Second year of 4 year transition on PE methodology – CMS is using results of 2009 AMA Physician Practice Information Survey • • – www. ama-assn. org/go/ppisurvey Neurology $73 PE/hr, $127. 21 Total PE/hr; Overall increase 3% • Neurosurgery $81 PE/hr, $132. 52 Total PE/hr; Overall increase 2% Assume that imaging equipment such as CT and MRI are used 90% of the time instead of current 50% – Other equipment remains at 50% usage for now – Work defined as 150, 000 minutes/year (48 hour work week)

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95812, EEG 41 -60 minutes – – Total RVUs: 9. 31, +28% Practice Expense: 8. 16, 33% Professional: 1. 60, +8% Physician Work (w. RVU): 1. 08, No change • 95813, EEG > 1 hour – – Total RVUs: 10. 48, +21% Practice Expense: 8. 64, 26% Professional: 2. 54, +7% Physician Work (w. RVU): 1. 73, No change

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95816, Awake EEG – – Total RVUs: 8. 39, +26% Practice Expense: 7. 22, 31% Professional: 1. 60, +8% Physician Work (w. RVU): 1. 08, No change • 95819, Awake and Asleep EEG – – Total RVUs: 9. 62, +32% Practice Expense: 8. 47, 38% Professional: 2. 54, +7% Physician Work (w. RVU): 1. 73, No change

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95822, Sleep EEG – – Total RVUs: 7. 84, +33% Practice Expense: 7. 22, +31% Professional: 1. 60, +8% Physician Work (w. RVU): 1. 08, No change • 95824, EEG for Brain Death – – Total RVUs: 0. 00, No change Practice Expense: 0. 00, N/A Professional: 1. 12, +8% Physician Work (w. RVU): 0. 74, No change

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95827, Overnight EEG – – Total RVUs: 16. 52, +33% Practice Expense: 15. 31, +36% Professional: 1. 60, +8% Physician Work (w. RVU): 1. 08, No change • 95829, Surgery Electrocorticogram – – Total RVUs: 44. 12 +20% Practice Expense: 37. 71, +29% Professional: 9. 11, +8% Physician Work (w. RVU): 6. 20, No change

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95950, Ambulatory Cassette EEG – Total RVUs: 7. 99, +18% – Practice Expense: 6. 38, +22% – Professional: 2. 25, +9% – Physician Work (w. RVU): 1. 51, No change • 95951, 24 Hour Video EEG – Total RVUs: 0. 00, *Carrier-defined technical expense – Practice Expense: *Carrier-defined technical expense – Professional: 9. 14, +8% – Physician Work (w. RVU): 5. 99, No change

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor Codes presented at RUC 04/2010 by M. Spanaki • 95953, 24 hour computerized digital EEG, unattended – Total RVUs: 12. 19, +6% – Practice Expense: 7. 56, +8. 78% – Professional: 4. 63, 1. 76% – Physician Work (w. RVU): 3. 08 • 95956, 24 Hour attended EEG without video – Total RVUs: 29. 82, 49. 92% – Practice Expense: 24. 6, 57. 19% – Professional: 5. 22, +23. 11% – Physician Work (w. RVU): 3. 61

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95954, EEG with administration of drugs – Total RVUs: 9. 15, +26. 56% – Practice Expense: 5. 8 RVUs, +41. 12% – Professional: 3. 35 RVUs, 7. 37% – Physician Work (w. RVU): 2. 45 • 95955, EEG during surgery – Total RVUs: 4. 96, 25. 89% – Practice Expense: 3. 48, 35. 41% – Professional: 1. 48, 8. 03% – Physician Work (w. RVU): 1. 01

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95957, EEG Digital Analysis – Total RVUs: 10. 01, +27. 68% – Practice Expense: 7. 05 RVUs, +41. 12% – Professional: 2. 96 RVUs, 8. 03% – Physician Work (w. RVU): 1. 98 • 95958, EEG monitoring, functional mapping (Wada Test) – Total RVUs: 13. 39, 20. 20% – Practice Expense: 7. 08, 34. 35% – Professional: 1. 48, 8. 03% – Physician Work (w. RVU): 4. 24

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95961, Electrode stimulation, brain, first hour – Total RVUs: 7. 41, +16. 88% – Practice Expense: 2. 93 RVUs, +33. 79% – Professional: 4. 48 RVUs, +7. 95% – Physician Work (w. RVU): 2. 97 • 95962, Electrode stimulation, brain, each additional hour – Total RVUs: 6. 67, +14. 21% – Practice Expense: 1. 8, +33. 33% – Professional: 4. 79, +8. 13% – Physician Work (w. RVU): 3. 21

2011 MFS for Neurology Services* *RVUs, excluding the conversion factor • 95970, Analyze neurostimulator, no programming – Physician Work (w. RVU): 0. 45 • 95975, Cranial neurostimulation, complex analysis and programming – Physician Work (w. RVU): 1. 70

2009 AAN MEG Payment Policy In 2008, AAN MEM Payment Policy Subcommittee decided to develop a model payment policy for MEG due to difficulties in getting MEG payments by insurers – Satya-Murti, William Sutherling, and Gregory L. Barkley wrote the policy – Joel Kaufman, M. D. & Katie Kuechenmeister lead AAN efforts – Passed by AAN Board of Directors on May 8, 2009 – Sent by AAN MEM to major insurance companies – http: //www. aan. com/globals/axon/assets/5641. pdf ACMEGS developed a similar policy in 2009 – Anto Bagic, Michael Funke, & John Ebersole wrote the policy – JClin. Neurophys 26 (4) p 290 -293, 2009 Model payment policy, letters, & meetings changed insurance coverage by major providers

Secrets to success in dealing with insurance companies Data, data, especially evidence-based The AAN & ACMEGS statements are referenced in the MEG policy review. I am certain that the AAN MEG policy review was a crucial piece of information in this change in policy – Several of the points in the AAN payment policy statement are restated in the AETNA review Personal Contacts and establishing relationships with the decision-makers were also key factors

CIGNA MEG Payment Policy #0248 For 12/15/2009 to 12/15/2010, “CIGNA does not cover magnetoencephalography (MEG) or magnetic source imaging (MSI) for any condition because they are considered experimental, investigational or unproven. ” The AAN MEM Payment Policy Subcommittee (PPS) met with CIGNA representatives in September 2010 CIGNA requested a letter regarding their policies AAN Response letter sent November 12, 2010 by Joel Kaufman, Chair of AAN PPS CIGNA has not yet posted MEG policy for 2011

2011 Medicare MEG Medicare Fee Schedule 95965 Spontaneous MEG for epileptic spike mapping 95966 Evoked magnetic fields 95967 Each additional evoked magnetic field procedure – 2011 Professional 12. 34 Total RVUs (7. 99 w. RVUs) • 2010 11. 83 Total RVUs (+8. 0%) Payment ? – 2011 Technical (APC 067) $3408. 69 (-4. 6 %) – 2011 Professional 6. 16 Total RVUs (3. 99 w. RVUs) 2010 5. 72 Total RVUs (+8, 0 %) Payment ? – Technical (APC 066) $977. 12 • 2010 $962. 61 (+1. 5 %) – 2011 Professional 5. 34 Total RVUs (3. 49 w. RVUs) • 2010 4. 92 Total RVUs (+9. 0 %) Payment ? – Technical (APC 066) $977. 12 • 2010 $962. 61 (+1. 5 %) * When one procedure is performed with another, payment would be reduced by 50% * Charges to private insurance are set by each laboratory and cannot be compared due to US antitrust (price-fixing) laws
 requires that CMS establish")
MEG Practice Expense Payment Rate The Affordable Care Act (ACA) requires that CMS establish the equipment utilization rate for CT, MR and PET at 75 percent. CMS had previously set the equipment utilization rate for this equipment at 90 percent, phasing in reduced payments over four years. This may result in changes to payment rates for CT and MR services. May affect MEG technical pricing since MEG grouped in imaging APCs

2010 e-Prescribing • PQRI revision for e-Rx – For 2011, only have to report at least 25 uses of e-Rx to qualify for PQRI payment – Failure to register for e-Rx in first half of 2011 and do not qualify for an exemption will face penalties in 2012. – – AAN has signed on to a letter of protest Physicians who participate in 2011 EHR cannot participate in e-Rx incentive program
 http: //www. cms. hhs. gov/apps/media/press/factsheet. asp? • AAN has")
PQRI (Physician Quality Reporting Initiative) http: //www. cms. hhs. gov/apps/media/press/factsheet. asp? • AAN has developed 8 epilepsy measures lead by N. Fountain and P Van Ness – Approved by AMA Physician's Consortium for Performance Improvement – Currently under review by National Quality Forum (NQF) – If NQF approves, then will be submitted to CMS for possible inclusion in the PQRI – Being developed by AAN for Maintenance of Certification program as a module

CPT Medicare Payment Relative to Site of Services Professional Component Technical Component Inpatient Use -26 modifier; Paid to physician Single DRG payment made to hospital to cover all technical expenses for that admission (IPPS) Outpatient medical center (includes EDs) Use -26 modifier; Paid to physician APC payment made to medical center (HOPPS) Outpatient, private office Global bill Submitted for professional and technical components Paid to physician

Mapping of Seizure/Epilepsy DRG Documentation Principle Diagnosis Seizure, psychogenic 780. 39 (other 101 Sz w MCC 100 Sz w/o MCC 345. 8 y 101 Sz w MCC 100 Sz w/o MCC nonepileptic seizure, spells Recurrent seizures, Epilepsy, Seizure disorder Specific epilepsies Psychogenic conversion disorder Secondary Diagnosis convulsions) (other recurrent seizures) MS DRG v 25 345. xy 300. 11 (Conversion disorder) 780. 39 880 Acute Adjustment Reaction
 Published 11/24/2010 – 782 pages in the")
2011 Hospital Outpatient Prospective Payment System (HOPPS) Published 11/24/2010 – 782 pages in the Federal Register – http: //edocket. access. gpo. gov/2010/pdf/2010 -27926. pdf Payment for the technical portion of CPT codes done on Medicare Outpatients Some outpatient procedures with HOPPS values have no payment assigned in MFS for doctors billing global – 95951 24 hour video EEG is “carrier priced” – 95965 MEG is “carrier priced” Payment for technical portion of Medicare inpatients is bundled into a single DRG payment Payment for technical fees in outpatients in private offices is in the Medicare Physician Fee Schedule • Billing “global” in private offices

2011 HOPPS APC 0213 • APC 0213 Level 1 Sleep, EEG, and CV studies – 95812 EEG 41 -60 min – 95812 EEG > 1 hour – 95816 EEG awake and drowsy – 95819 EEG awake and asleep – 96822 EEG sleep and/or coma – 95827 EEG all night recording – 95958 EEG monitoring/function test • 2010 APC rate is $162. 06 • 2011 APC rate will be $166. 64 • Increase of $4. 62 or 2. 83%

2011 HOPPS APC 0209 • APC 0209 Level II sleep, EEG, & CV – – – 95950 ambulatory cassette EEG 95951 24 hour video EEG 95953 ambulatory digital EEG 95956 24 hour EEG without video MSLP and polysomnograms • 2010 APC Rate is $770. 55 • 2011 APC Rate will be $780. 77 • Increase of $10. 22 or 1. 33%

2011 HOPPS APC 218 • APC 218 Level II Nerve and Muscle Tests – 95970 Neurostimulation, analysis with no programming – 95954 EEG monitoring with drug administration • 2010 payment is $80. 65 • 2011 payment will be $80. 78 • Increase of $0. 13 or 0. 16%

2011 HOPPS APC 216 • APC 216 Level III Nerve and Muscle Tests – – 95961 Cortical Stimulation, 1 st hour 95962 Cortical Stimulation, each additional hour • 2010 payment is $180. 86 • 2011 payment will be $186. 17 • Increase of $5. 31 or 2. 94%

2011 HOPPS APC 0692 • APC 0692 Level III Electronic Analysis of Devices – 95971 Analyze neurostim, simple – 95972 Analyze neurostim, complex – 95973 Analyze neurostim, complex – 95974 Cranial neurostim, complex – 95978 Analyze neurostim brain, 1 st hour – 95979 Analyze neurostim brain, each 1 hour – 95982 Low gain neurostim subseq w/ reprogram • 2010 payment is $107. 85 • 2011 payment will be $110. 95 • Increase of $3. 10 or 2. 87%

2011 MEG HOPPs Technical payments for MEG studies in hospitalbased outpatient care facilities – Does not apply to free standing MEG sites • Carrier priced – Does not apply to MEG studies done on inpatients • Technical fees bundled to DRG

2010 HOPPS APC 0067 • APC 0065 Level III Stereotactic Radiosurgery, MRg. FUS, and MEG – 95965 MEG, spontaneous • 2010 payment is $3571. 78 • 2011 payment is $3408. 69 • Decrease of $163. 09 or 4. 57% • Caught by the change in assumption of work hours for equipment costing more than $1 M. Decrease of $394. 54 in past two years. • New MEG cost reporting may help – MEG and EEG were combined on Line 54 of the Medicare Cost Report – Now MEG is moved to a new line, 54. 01

2011 HOPPs APC 0065 Level I Stereotactic radiosurgery, Mrg. GUS, and MEG – 95966 MEG Evoked Response – 95967 Additional MEG Evoked Response 2010 payment is $962. 61 2011 payment will be $977. 12 Increase of $14. 51 or 1. 5%

Update on HFHS Transition to ICD-10 Coding System Kickoff: December 9, 2010 Nov 18 th , 2010
 Final Rule: HHS published on Jan 2009 Compliance")
ICD-10 -CM/PCS (Clinical Modification/Procedure Coding System) Final Rule: HHS published on Jan 2009 Compliance Date: October 1 st, 2013 • ICD-10 -CM/PCS will enhance accurate payment for services rendered and facilitate evaluation of medical processes and outcomes. • ICD-10 -CM – The diagnosis classification system developed by the Centers for Disease Control and Prevention for use in all (inpatient and outpatient) U. S. health care treatment settings. Diagnosis coding under this system uses 3– 7 alpha and numeric digits and full code titles, but the format is very much the same as ICD-9 -CM • ICD-10 -PCS – The procedure classification system developed by the Centers for Medicare & Medicaid Services (CMS) for use in the U. S. for inpatient hospital settings ONLY. The new procedure coding system uses 7 alpha or numeric digits while the ICD-9 -CM coding system uses 3 or 4 numeric digits. • A number of other countries have already moved to ICD-10, including: – – – United Kingdom (1995); France (1997); Australia (1998); Germany (2000); and Canada (2001). 65

HIPAA X 12 5010 Electronic Transaction Changes • All HIPAA X 12 Electronic Transactions with payors (e. g. , eligibility verification, claims, remittance advise) have to be upgraded from current 4010 version to newer 5010 version • This will enable payors to request more information in the future electronic transactions (adding extra lanes to electronic freeway system to carry more information) • This change has to be operational by Jan 1 2012 and it is a prerequisite for ICD 10 CM/PCS changes 66

ICD-9 -CM - Shortcomings • Shortcomings of ICD-9 include: – ICD-9 is outdated, with only a limited ability to accommodate new procedures and diagnoses; – ICD-9 lacks the precision needed for a number of emerging uses such as payfor-performance and biosurveillance. Biosurveillance is the automated monitoring of information sources that may help in detecting an emerging epidemic, whether naturally occurring or as the result of bioterrorism; – ICD-9 limits the precision of diagnosis-related groups (DRGs) as a result of very different procedures being grouped together in one code; – ICD-9 lacks specificity and detail, uses terminology inconsistently, cannot capture new technology, and lacks codes for preventive services; and – ICD-9 will eventually run out of space, particularly for procedure codes. 67

Expected Benefits from usage of ICD 10 codes • Adoption of the ICD-10 code sets is expected to: – Support value-based purchasing and Medicare’s anti-fraud and abuse activities by accurately defining services and providing specific diagnosis and treatment information; – Support comprehensive reporting of quality data; – Ensure more accurate payments for new procedures, fewer rejected claims, improved disease management, and harmonization of disease monitoring and reporting worldwide; and – Allow the United States to compare its data with international data to track the incidence and spread of disease and treatment outcomes because the United States is one of the few developed countries not using ICD-10. 68

Next Generation of Coding Structural Changes S. No. ICD-9 -CM ICD-10 -CM / PCS 1. Minimum of 3 digits, maximum of 5 digits, decimal point after the third digit Minimum of 3 digits, maximum of 7 digits, decimal point after the third digit 2. Numeric, except for supplementary codes — V codes and E codes Alphanumeric, with all codes using alphabetic lead character; V and E codes have been eliminated and incorporated into the main code set 3. Structure of injuries designated by wound type Structure of injuries designated by body part (location) 4. Diagnosis: 13, 000 Codes IP Procedure: 4, 000 Codes 67, 000 ICD-10 -CM Codes 87, 000 ICD-10 -PCS Codes Mapping – ICD-9 To ICD-10 One to One: One old code to one new code. 3, 458 codes or 24. 52 % of all ICD-9 DX codes Single Entry: One old code to one of many new code. 9, 600 codes or 68. 07 % of all ICD-9 DX codes Combination Entry: One old code is split into multiple new code. 629 codes or 4. 46 % of all ICD-9 DX codes No Match: All new codes. 416 codes or 2. 95 % of all ICD-9 DX codes 69

Difference between ICD-9 and ICD-10 ICD-9 -CM Mechanical complication of other vascular device, implant and graft 1 code (996. 1) ICD-10 -CM Mechanical complication of other vascular grafts 156 codes, including T 82. 310 – Breakdown (mechanical) of aortic (bifurcation) graft (replacement) T 82. 311 – Breakdown (mechanical) of carotid arterial graft (bypass) T 82. 312 – Breakdown (mechanical) of femoral arterial graft (bypass) T 82. 318 – Breakdown (mechanical) of other vascular grafts T 82. 319 – Breakdown (mechanical) of unspecified vascular grafts T 82. 320 – Displacement of aortic (bifurcation) graft (replacement) T 82. 321 – Displacement of carotid arterial graft (bypass) T 82. 322 – Displacement of femoral arterial graft (bypass) ICD-9 -CM Angioplasty 1 code (39. 50) ICD-10 -PCS Angioplasty codes 854 codes Specifying body part, approach, and device, including: 047 K 04 Z – Dilation of right femoral artery with drug-eluting intraluminal device, open approach 047 K 0 DZ – Dilation of right femoral artery with intraluminal device, open approach 047 K 0 ZZ – Dilation of right femoral artery, open approach 047 K 34 Z – Dilation of right femoral artery with drug-eluting intraluminal device, percutaneous approach 047 K 3 DZ – Dilation of right femoral artery with intraluminal device, percutaneous Approach T 82. 328 – Displacement of other vascular grafts 70

ICD-10 Example Fracture of wrist • Patient fractures left wrist • A month later, fractures right wrist • ICD-9 -CM does not identify left versus right (requires additional documentation to clarify during claim adjudication) • ICD-10 -CM describes left versus right, Initial encounter, subsequent encounter, routine healing, delayed healing, nonunion, or malunion 71

Potential Risks of Transition to ICD 10 • Training and Education – ICD 10 codes are based on human anatomy and physiology will require significant mind set change for coders to get used to new system • Business Process – Potential significant shift in roles and responsibilities between clinicians and coders to handle the complexity of ICD 10 s • Information Technology – Significant risk in modifications to several systems to accommodate new code sets • Financial/Reimbursement – Transition from ICD 9 to ICD 10 can result into temporary delays in cash flow from payors due to technology implementation glitches 72


ICD 10 Potential Impacts to HFMG Operations • Significant process changes in the areas of documentation, coding and charge capture • May result in extensive training for Physicians, Coders and other care-givers • Medi. Pac revenue cycle systems will be modified to address transition to ICD 10 • OMR and TCAP systems have to be replaced with newer technology to handle the complexity and explosion of ICD 10 codes 74

OMR Considerations • HFMG Clinic Coding model: Physician Model enabled by branching technology logic (CAC) vs. Centralized Coder model • Handheld devices with future integration with Care. Plus(NG)/CPOE solution 75

HFHS ICD-10 Project Phasing Phase 1 – Impact Assessment & Planning • • • Develop project management structure Engage Steering Committee and Business Unit Operational Teams Assess Process Implications Assess IT Systems impact Create Multi-Year Capital and Expense budget to address the change Phase 2 – Process Redesign and IT System Changes • Process Redesign-Current and Future State • Detailed analysis, design and build of IT changes • Create testing plans to validate process redesign and IT system changes 76

HFHS ICD-10 Project Phasing Phase 3 – Testing and Implementation Planning • Internal Testing and Training • External Testing (Payors, Regulatory Reporting) • Operational Readiness and Implementation Planning Phase 4 – End User Training and Go-Live • Finalize IT system changes and certify testing • Finalize process changes and certify operational readiness • Complete intensive coding professional education Phase 5 – Post Go-Live Support • Monitor coding accuracy for reimbursement, coding productivity and continue with appropriate coding professional training 77

HFHS Project Phasing and Tentative Timeline 78
 • History of")
Key components of level of service History • Chief complaint (CC) • History of present illness (HPI) • Past medical, family, social history (PFSH) • Review of systems (ROS) Examination • Neurological single system exam or general multi-system exam Medical Decision Making • Number of diagnoses or number of management options • Complexity of data • Risk of morbidity and mortality

You Get Credit for Trying. . . • Sometimes, you cannot do a full H & P no matter what – • History – • Document your attempt and what happened Patient aphasic, lethargic, in coma, won't answer, demented, etc. PE – Patient aphasic, uncooperative, limb amputated, strict bedrest, etc. • Do not write “unable to obtain” • Forgetting one bullet point on a New Patient visit has major consequences in billing: drops to a level 1 visit

Tips for documenting history • CC always required • ROS is very important – must document pertinent positives, may be in HPI – “all other systems negative” permitted – ROS deficiency a major reason for not meeting criteria for highest level of service • ROS and PFSH – staff may record, and physician note – may use previous ROS and PFSH, revise as needed • If history not obtainable, document why
 1997 E &M Guidelines allow for the option of")
History of Present Illness (HPI) 1997 E &M Guidelines allow for the option of documenting the status/acuity of chronic problems and/or inactive problems to complete the History of Present Illness. IMPORTANT: You must document the chronic or inactive problem that you are addressing during the visit and detail the current status/acuity of the problem
 of the neuro")
Documenting the neurological examination • CPT™ defines 25 individual elements (“bullets”) of the neuro exam, in 4 main groups – – constitutional, eyes, cardiovascular higher integrative functions or mental status cranial nerves musculoskeletal, motor, and sensory • CPT™ specifies the numbers of elements that must be documented for each level of service • You must comment on these elements (“WNL” not acceptable)
 Documentation Tips • Document the test(s) that you have reviewed")
Medical Decision Making (MDM) Documentation Tips • Document the test(s) that you have reviewed (summarize what you have reviewed) and ordered • Document discussing test(s) with the physician who performed the test. For example discussing with the cardiologist the interpretation of an echocardiogram • Document the review of old records. Remember you must summarize what you have reviewed. • For Example: Patient was admitted a month ago for _____. Course of treatment included ____and patient was discharged with home health care and continue with _____. IF IT IS NOT DOCUMENTED IT IS NOT DONE
 Medical decision making refers to the complexity of establishing a")
Medical Decision Making (MDM) Medical decision making refers to the complexity of establishing a diagnosis and/or selecting a management option. It can be broken down into three components. – Number of diagnoses or management options – Amount and complexity of data to review (Previous documentation tips support this component) – Risk of complication and/or morbidity or mortality

2002 CMS Regulations on Supervision of Residents and Students • Effective date November, 22, 2002 • Resident means an individual who participates in an approved graduate medical education (GME) program • Receiving a staff or faculty appointment or participating in a fellowship does not by itself alter the status of “resident”. • A student is never considered to be an intern or a resident. Medicare does not pay for any clinical service furnished by a student. (Medicare pays hospitals and medical schools large sums of money in other ways. )
 of")
Medicare Teaching Definitions • Critical or key portion means that part (or parts) of a service that the teaching physician determines is (are) a critical or key portion(s). • Documentation may be dictated and typed, handwritten or computer-generated, and typed or handwritten. • Documentation must be dated and include a legible signature or identity.

Payment Definitions • For purposes of payment, E/M services billed by teaching physicians require that they personally document at least the following: – a. That they performed the service or were physically present during the key or critical portions of the service when performed by the resident; and – b. The participation of the teaching physician in the management of the patient. • When assigning codes to services billed by teaching physicians, reviewers will combine the documentation of both the resident and the teaching physician. • Documentation for the service must support the medical necessity of the service.

Examples of Acceptable Notes • “I was present with resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note. ” • “I saw the patient with the resident and agree with the resident’s findings and plan. ” • “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written. ” • “I saw and evaluated the patient. Agree with resident’s note but lower extremities are weaker, now 3/5; MRI of L/S Spine today. ”

Examples of Unacceptable Notes • • • “Agree with above. ” “Rounded, Reviewed, Agree” “Discussed with resident. Agree. ” “Seen and agree. ” “Patient seen and evaluated” A legible countersignature or identity alone.

E/M Service Documentation Provided By Students. • Any contribution and participation of a student to the performance of a billable service (other than the review of systems and/or past family/social history which are not separately billable, but are taken as part of an E/M service) must be performed in the physical presence of a teaching physician or physical presence of a resident in a service meeting the requirements set forth in this section for teaching physician billing.

E/M Service Documentation Provided By Students. • Students may document services in the medical record. • Documentation by a student that may be referred to by the teaching physician is limited to the review of systems and/or past family/social history. • The teaching physician may not refer to a student’s documentation of physical exam findings or medical decision making in his or her personal note. • The teaching physician must verify and redocument the history of present illness as well as perform and redocument the physical exam and medical decision making activities of the service.

DISCHARGE DAY • On the day of discharge, code as follows: – 99238 for a total staff time of 30 minutes or less – • 99239 for a total staff time of more than 30 minutes You must document the time spent in your note – Time does not need to be continuous – Time does not need to be spent with the patient and includes: • • • Writing Rx Doing discharge summary Making follow up arrangements Contacting other providers Resident time does not count
942fc595ea835fdd0d273a819513ae0f.ppt