

db3e5cd9c6c414c80f1312633fa2c64b.ppt
- Количество слайдов: 64
 Adherence Tools of Yesterday, Today and Tomorrow Seth Heldenbrand, Pharm. D. Associate Professor University of Arkansas for Medical Sciences
Adherence Tools of Yesterday, Today and Tomorrow Seth Heldenbrand, Pharm. D. Associate Professor University of Arkansas for Medical Sciences
 Disclosure • Financial disclosures – I have no financial conflicts to disclose
Disclosure • Financial disclosures – I have no financial conflicts to disclose
 Objectives 1. Summarize adherence terminology/epidemiology 2. Identify risk factors for non-adherence and tools to measure it 3. Evaluate traditional methods used to improve/monitor medication adherence 4. Review today’s technologies for improving/monitoring medication adherence 5. Summarize tomorrow’s technologies for improving/monitoring medication adherence
Objectives 1. Summarize adherence terminology/epidemiology 2. Identify risk factors for non-adherence and tools to measure it 3. Evaluate traditional methods used to improve/monitor medication adherence 4. Review today’s technologies for improving/monitoring medication adherence 5. Summarize tomorrow’s technologies for improving/monitoring medication adherence
 Definition of Adherence • Compliance – “the extent to which a patient’s behavior matches the prescriber’s recommendation” • Adherence – “the extent to which the patient’s behavior matches the agreed upon prescriber’s recommendation” Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41
Definition of Adherence • Compliance – “the extent to which a patient’s behavior matches the prescriber’s recommendation” • Adherence – “the extent to which the patient’s behavior matches the agreed upon prescriber’s recommendation” Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41
? • “Deviation from the prescribed medication regimen sufficient to") So What Is Nonadherence (NA)? • “Deviation from the prescribed medication regimen sufficient to influence adversely the regimen’s intended effect”. Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41
So What Is Nonadherence (NA)? • “Deviation from the prescribed medication regimen sufficient to influence adversely the regimen’s intended effect”. Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41
 NA In the U. S. • Adversely affects health • Negative impact on relationship with health care provider • Skew results of clinical trials • Increases health resource consumption
NA In the U. S. • Adversely affects health • Negative impact on relationship with health care provider • Skew results of clinical trials • Increases health resource consumption
 Epidemiology of NA • General population – 33 -69% of medication related hospitalizations – $100 billion annually – Adherence to chronic medications is approximately 50% Dayer, L. , Heldenbrand, S. , Anderson, P. , Gubbins, P. O. , & Martin, B. C. (2013). Smartphone medication adherence apps: potential benefits to patients and providers. Journal of the American Pharmacists Association, 53(2), 172 -181.
Epidemiology of NA • General population – 33 -69% of medication related hospitalizations – $100 billion annually – Adherence to chronic medications is approximately 50% Dayer, L. , Heldenbrand, S. , Anderson, P. , Gubbins, P. O. , & Martin, B. C. (2013). Smartphone medication adherence apps: potential benefits to patients and providers. Journal of the American Pharmacists Association, 53(2), 172 -181.
 Measurement of Adherence • Direct – Observation of ingestion • Physical or electronic • Indirect – Patient self-reports – Pill counts – Refill rates – Blood monitoring – Electronic monitoring What are the drawbacks to these indirect methods?
Measurement of Adherence • Direct – Observation of ingestion • Physical or electronic • Indirect – Patient self-reports – Pill counts – Refill rates – Blood monitoring – Electronic monitoring What are the drawbacks to these indirect methods?
 Types of NA • Intentional – Rational decision • Beliefs/feelings • Unintentional – Intending to take the medication • Forgetfulness • Carelessness • Financial
Types of NA • Intentional – Rational decision • Beliefs/feelings • Unintentional – Intending to take the medication • Forgetfulness • Carelessness • Financial
 Risk Factors for NA • • • History of NA Psychiatric illness Personality disorders Substance abuse Adolescence Chronic illness Physician communication Illiteracy Low self efficacy • • • Side effects Cost Complex regimen Poor aftercare/discharge Negative beliefs in medications • Socioeconomic status • History of abuse • Race/culture Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41
Risk Factors for NA • • • History of NA Psychiatric illness Personality disorders Substance abuse Adolescence Chronic illness Physician communication Illiteracy Low self efficacy • • • Side effects Cost Complex regimen Poor aftercare/discharge Negative beliefs in medications • Socioeconomic status • History of abuse • Race/culture Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41
 Methods to Improve Adherence • Behavioral – Reminder systems • Educational – Counseling reinforcement • Organizational – Decreasing regimen complexity • Removing barriers – $$$
Methods to Improve Adherence • Behavioral – Reminder systems • Educational – Counseling reinforcement • Organizational – Decreasing regimen complexity • Removing barriers – $$$
 Medication Adherence Aids • Traditional – Best for unintentional NA • Pill boxes, unit-of-use packaging, alarms – Minimally involves patient in the process – Provide no adherence data – Many are passive systems
Medication Adherence Aids • Traditional – Best for unintentional NA • Pill boxes, unit-of-use packaging, alarms – Minimally involves patient in the process – Provide no adherence data – Many are passive systems
 Behavioral Interventions • Patient education – Best method to improve adherence – Especially for those taking more than six medications • Emotional intelligence • Motivational interviewing
Behavioral Interventions • Patient education – Best method to improve adherence – Especially for those taking more than six medications • Emotional intelligence • Motivational interviewing
 New and Emerging Adherence Technologies • Mobile Adherence Applications “Apps” • Internet-connected adherence monitoring technologies • Electronic and biometric ingestion confirming technologies
New and Emerging Adherence Technologies • Mobile Adherence Applications “Apps” • Internet-connected adherence monitoring technologies • Electronic and biometric ingestion confirming technologies
 Improving Adherence In Your Patients 1. NA is multifactorial 2. Interventions should be customized for each patient and pattern of NA 3. Foundation should be educational and behavior modifying 4. Multiple approaches should be used simultaneously
Improving Adherence In Your Patients 1. NA is multifactorial 2. Interventions should be customized for each patient and pattern of NA 3. Foundation should be educational and behavior modifying 4. Multiple approaches should be used simultaneously
 Traditional Adherence Tools
Traditional Adherence Tools
 Traditional Adherence Tools 1. 2. 3. 4. 5. Counseling/Education Regimen books “black books” Regimen print outs Administration check lists Pill boxes (and other pill reminder tools)
Traditional Adherence Tools 1. 2. 3. 4. 5. Counseling/Education Regimen books “black books” Regimen print outs Administration check lists Pill boxes (and other pill reminder tools)
 Counseling/Education • Time intensive • Health literacy concerns – – – Communication skills (YOURS and theirs) Knowledge of health topics (YOURS and theirs) Culture Barriers to health system/care Demands of situation/context Education in non-health areas (reading, math, general education level)
Counseling/Education • Time intensive • Health literacy concerns – – – Communication skills (YOURS and theirs) Knowledge of health topics (YOURS and theirs) Culture Barriers to health system/care Demands of situation/context Education in non-health areas (reading, math, general education level)
 Clear Communication 1. 2. 3. 4. 5. 6. 7. 8. 9. Warm greeting Eye contact Plain, non-medical language Slow down Limit content (3 -5 points) Repeat key points Graphics (when applicable) Patient participation Teach-back
Clear Communication 1. 2. 3. 4. 5. 6. 7. 8. 9. Warm greeting Eye contact Plain, non-medical language Slow down Limit content (3 -5 points) Repeat key points Graphics (when applicable) Patient participation Teach-back
 Teach-back Method • What percentage of medical information if forgotten immediately – 40 -80% • What percentage of information retained is incorrect? – Almost 50% • Teach-back involves asking the patient to repeat what you have just told them • Repeat the process until they get it right • Confirms patient understanding of instructions
Teach-back Method • What percentage of medical information if forgotten immediately – 40 -80% • What percentage of information retained is incorrect? – Almost 50% • Teach-back involves asking the patient to repeat what you have just told them • Repeat the process until they get it right • Confirms patient understanding of instructions
 Teach-back Method • Not a test of the patient knowledge – It is a test of how well you explained the concept • Use with everyone – Even when you think they understood • Should be used by all medical staff – MD/RN/Pharm. D/everyone
Teach-back Method • Not a test of the patient knowledge – It is a test of how well you explained the concept • Use with everyone – Even when you think they understood • Should be used by all medical staff – MD/RN/Pharm. D/everyone
 • Reinforcing action plans") Follow-up with Patients • Monitoring health (BP, blood sugar, weight) • Reinforcing action plans • Assessing/Confirming adherence • Verifying follow-through on referrals • Communicating lab results
Follow-up with Patients • Monitoring health (BP, blood sugar, weight) • Reinforcing action plans • Assessing/Confirming adherence • Verifying follow-through on referrals • Communicating lab results
 “Black Books” 1. Contact info 2. Brand/Generic 3. Each med is a card 4. Pencil 5. Patient’s responsibility
“Black Books” 1. Contact info 2. Brand/Generic 3. Each med is a card 4. Pencil 5. Patient’s responsibility
 Medication Regimens www. medactionplan. com 1. Brand generic names 2. Pictures of the meds 3. Drug, strength, dose, time 4. Contact information www. medactionplan. com
Medication Regimens www. medactionplan. com 1. Brand generic names 2. Pictures of the meds 3. Drug, strength, dose, time 4. Contact information www. medactionplan. com
 Administration Checklists • Continues inpatient administration procedure as an outpatient • Not for every patient • “Type A” comes to mind… www. medactionplan. com
Administration Checklists • Continues inpatient administration procedure as an outpatient • Not for every patient • “Type A” comes to mind… www. medactionplan. com
 2. Weekly pillboxes ($11. 24) 3. Electronic") Traditional Reminders 1. Daily pillbox ($2. 49) 2. Weekly pillboxes ($11. 24) 3. Electronic pillboxes ($13. 99) 4. Wearable digital reminder alarms ($139. 95)
Traditional Reminders 1. Daily pillbox ($2. 49) 2. Weekly pillboxes ($11. 24) 3. Electronic pillboxes ($13. 99) 4. Wearable digital reminder alarms ($139. 95)
 2. Multi-Alarm Time. Cap ($29. 95)") Other Adherence Tools 1. Multi-Alarm Pocket ($39. 95) 2. Multi-Alarm Time. Cap ($29. 95) 3. MEDglider 4 Alarm Pillbox ($45. 95) 4. Compu. Med Automated Dispenser ($895)
Other Adherence Tools 1. Multi-Alarm Pocket ($39. 95) 2. Multi-Alarm Time. Cap ($29. 95) 3. MEDglider 4 Alarm Pillbox ($45. 95) 4. Compu. Med Automated Dispenser ($895)
 Other Adherence Tools 1. MEMS 6 Track. Cap ($107 for Track. Cap; $365 for reader) 2. Senticare Pill. Station ($89 enrollment; $79 per month) 3. Glow. Caps (discussed later)
Other Adherence Tools 1. MEMS 6 Track. Cap ($107 for Track. Cap; $365 for reader) 2. Senticare Pill. Station ($89 enrollment; $79 per month) 3. Glow. Caps (discussed later)
 Mobile Adherence Technologies “Apps”
Mobile Adherence Technologies “Apps”
 J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 Adherence Apps • Using a smartphone to improve adherence is still a novel approach 1. Consolidates health information onto one ubiquitous device 2. Little to no cost to the patient 3. Simplifies complex regimens 4. Literature on health and wellness is growing 5. Adherence data is lacking (although some promising results) J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
Adherence Apps • Using a smartphone to improve adherence is still a novel approach 1. Consolidates health information onto one ubiquitous device 2. Little to no cost to the patient 3. Simplifies complex regimens 4. Literature on health and wellness is growing 5. Adherence data is lacking (although some promising results) J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 2012 App Study Valuable App Attributes • Online data entry • Complex instruction capable • Cloud data storage • Searchable database of medications • Sync/export/print data • Tracks missed and taken doses • Provider data input capable • Multi-platform app • HIPAA compliant • Multiple profile feature • Multilingual J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
2012 App Study Valuable App Attributes • Online data entry • Complex instruction capable • Cloud data storage • Searchable database of medications • Sync/export/print data • Tracks missed and taken doses • Provider data input capable • Multi-platform app • HIPAA compliant • Multiple profile feature • Multilingual J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 2012 App Study Methods • Inclusion – i. Phone, Android, Blackberry OSs – English language – Must generate reminders • Exclusion – Designed for one medication type – Designed single disease state – Lacked description of functionality J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
2012 App Study Methods • Inclusion – i. Phone, Android, Blackberry OSs – English language – Must generate reminders • Exclusion – Designed for one medication type – Designed single disease state – Lacked description of functionality J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 • Scored and ranked") 2012 App Study Results • 160 apps reviewed (147 unique) • Scored and ranked based on author point system • Ten highest ranked apps were tested on available operating systems • Apps were evaluated against developer claims J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
2012 App Study Results • 160 apps reviewed (147 unique) • Scored and ranked based on author point system • Ten highest ranked apps were tested on available operating systems • Apps were evaluated against developer claims J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 And. (%) All apps BB (%) Total (%) 61 (38.") Attribute i. Phone (%) And. (%) All apps BB (%) Total (%) 61 (38. 1) 84 (52. 5) 15 (9. 4) 160 (100) Online entry 2 (3. 3) 8 (9. 5) 1 (6. 7) 11 (6. 9) Complex sig 12 (19. 7) 7 (8. 3) 2 (13. 3) 21 (13. 1) Cloud storage 4 (6. 6) 5 (6) 2 (13. 3) 11 (6. 9) Database of meds 4 (6. 6) 6 (7. 1) 0 (0) 10 (6. 3) Sync/export 22 (36. 1) 16 (19) 1 (6. 7) 39 (24. 4) Tracks doses 23 (37. 7) 19 (22. 6) 5 (33. 3) 47 (29. 4) Provider input 1 (1. 6) 2 (2. 4) 0 (0) 3 (1. 9) Multi-platform 11 (18) 12 (14. 3) 2 (13. 3) 25 (15. 6) HIPAA 2 (3. 3) 3 (3. 6) 0 (0) 5 (3. 1) Multi-profile 20 (32. 8) 13 (15. 5) 3 (20) 36 (22. 5) Multilingual 13 (21. 3) 9 (10. 7) 0 (0) 22 (13. 8) $2. 21 $2. 18 $4. 10 $2. 83 Average Price J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
Attribute i. Phone (%) And. (%) All apps BB (%) Total (%) 61 (38. 1) 84 (52. 5) 15 (9. 4) 160 (100) Online entry 2 (3. 3) 8 (9. 5) 1 (6. 7) 11 (6. 9) Complex sig 12 (19. 7) 7 (8. 3) 2 (13. 3) 21 (13. 1) Cloud storage 4 (6. 6) 5 (6) 2 (13. 3) 11 (6. 9) Database of meds 4 (6. 6) 6 (7. 1) 0 (0) 10 (6. 3) Sync/export 22 (36. 1) 16 (19) 1 (6. 7) 39 (24. 4) Tracks doses 23 (37. 7) 19 (22. 6) 5 (33. 3) 47 (29. 4) Provider input 1 (1. 6) 2 (2. 4) 0 (0) 3 (1. 9) Multi-platform 11 (18) 12 (14. 3) 2 (13. 3) 25 (15. 6) HIPAA 2 (3. 3) 3 (3. 6) 0 (0) 5 (3. 1) Multi-profile 20 (32. 8) 13 (15. 5) 3 (20) 36 (22. 5) Multilingual 13 (21. 3) 9 (10. 7) 0 (0) 22 (13. 8) $2. 21 $2. 18 $4. 10 $2. 83 Average Price J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 2012 Rank Post-testing 1. My. Med. Schedule 2. My. Meds 3. Med. Simple 4. Med Agenda (i. OS only) 5. Rxmind. Me (i. OS only) 6. Dosecast 7. TRx. C (Beta) 8. Medi. Memory (i. OS only) 9. Pill. Manager 10. Meds. IQ Individual/Multi-User (Android only) J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
2012 Rank Post-testing 1. My. Med. Schedule 2. My. Meds 3. Med. Simple 4. Med Agenda (i. OS only) 5. Rxmind. Me (i. OS only) 6. Dosecast 7. TRx. C (Beta) 8. Medi. Memory (i. OS only) 9. Pill. Manager 10. Meds. IQ Individual/Multi-User (Android only) J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 • Similar Inclusion and Exclusion criteria • Modified “important features”") 2014 App Study (Preliminary) • Similar Inclusion and Exclusion criteria • Modified “important features” • Tested the top 100 scoring apps
2014 App Study (Preliminary) • Similar Inclusion and Exclusion criteria • Modified “important features” • Tested the top 100 scoring apps
 • 461 apps reviewed (329 unique) • Scored and ranked") 2014 App Study (Preliminary) • 461 apps reviewed (329 unique) • Scored and ranked based on author point system • 100 highest ranked apps were tested on available operating systems • Apps were evaluated for real world performance against developer claims
2014 App Study (Preliminary) • 461 apps reviewed (329 unique) • Scored and ranked based on author point system • 100 highest ranked apps were tested on available operating systems • Apps were evaluated for real world performance against developer claims
 Total Apps 2012 - 2014
Total Apps 2012 - 2014
 Apps by OS 2012 - 2014
Apps by OS 2012 - 2014
 • What did we learn? – The adherence app market") 2014 App Study (Preliminary) • What did we learn? – The adherence app market place is exploding – It is difficult for patients to choose quality apps – Most “free” apps are not worth the effort • Limited functionality (bait apps) • Poorly finished • Packed with adds – False claims by developers
2014 App Study (Preliminary) • What did we learn? – The adherence app market place is exploding – It is difficult for patients to choose quality apps – Most “free” apps are not worth the effort • Limited functionality (bait apps) • Poorly finished • Packed with adds – False claims by developers
 Selecting the right app • Developing an adherence app website – Lets patient or provider select desired functions – Ranks apps by our features/testing formula by desired features – Eliminates the trial and error approach to medication adherence apps that exists now
Selecting the right app • Developing an adherence app website – Lets patient or provider select desired functions – Ranks apps by our features/testing formula by desired features – Eliminates the trial and error approach to medication adherence apps that exists now
 – 14 -42%") Future Directions for Apps • Growing smartphone use (55% in US) – 14 -42% persons age 65 or older • Companion websites for patients and providers • Escalating reminder systems • Tailored reminder systems – Motivating reminders – Less intrusive reminders for the adherent patient J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
Future Directions for Apps • Growing smartphone use (55% in US) – 14 -42% persons age 65 or older • Companion websites for patients and providers • Escalating reminder systems • Tailored reminder systems – Motivating reminders – Less intrusive reminders for the adherent patient J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 Future Directions for Apps • Connectivity: Real-time adherence info • Interconnectivity: synced hospital info, discharge instructions, pharmacy records • Medical social networks: patient specified providers apps contact at NA thresholds • Integration with ingestion sensor systems: the “holy grail” of adherence measurement J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
Future Directions for Apps • Connectivity: Real-time adherence info • Interconnectivity: synced hospital info, discharge instructions, pharmacy records • Medical social networks: patient specified providers apps contact at NA thresholds • Integration with ingestion sensor systems: the “holy grail” of adherence measurement J Am Pharm Assoc. 2013; 53: 172– 181. doi: 10. 1331/JAPh. A. 2013. 12202
 Emerging and Available Adherence Technologies
Emerging and Available Adherence Technologies
 • Caps communicate with base to") Glow. Caps www. glowcaps. com • Cellular (AT&T) • Caps communicate with base to track adherence • Progressive reminders 1. 2. 3. 4. 5. 6. Light up (cap) Light up (base) Play ringtone Call/text patient Requests Rx refills Weekly adherence report
Glow. Caps www. glowcaps. com • Cellular (AT&T) • Caps communicate with base to track adherence • Progressive reminders 1. 2. 3. 4. 5. 6. Light up (cap) Light up (base) Play ringtone Call/text patient Requests Rx refills Weekly adherence report
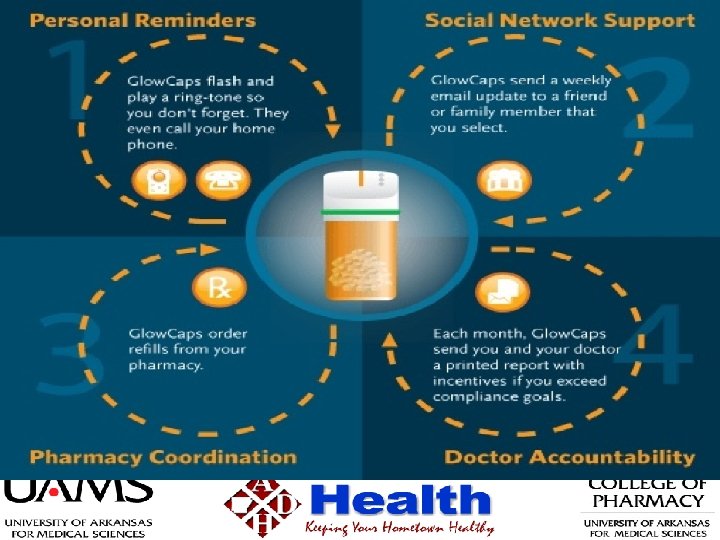
 Glow. Caps • Cost – $10 per cap – $15 per month AT&T • Results – Single study • Improved adherence from 71% to 98% – Other studies pending or unpublished – Current trials underway in transplant recipients
Glow. Caps • Cost – $10 per cap – $15 per month AT&T • Results – Single study • Improved adherence from 71% to 98% – Other studies pending or unpublished – Current trials underway in transplant recipients
 • Once a") • 6 month study randomized (nearing completion and publication hopefully) • Once a day meds for HTN • 27% increase in adherence over the control group (early results) • Funded by Glow. Caps
• 6 month study randomized (nearing completion and publication hopefully) • Once a day meds for HTN • 27% increase in adherence over the control group (early results) • Funded by Glow. Caps
 Similar Electronic Cap Technologies • e. CAP – Beeps and flashes – RFID communication • MEMS 6 Track. Cap – Records • bottle openings • uploads via reader
Similar Electronic Cap Technologies • e. CAP – Beeps and flashes – RFID communication • MEMS 6 Track. Cap – Records • bottle openings • uploads via reader
 Med. Minder www. medminder. com • 7 day pill box – Cellular connectivity • Lights up and beeps when a dose is due • Central database records adherence • Missed doses trigger calls, texts, email • Social involvement (MD, caregiver, etc)
Med. Minder www. medminder. com • 7 day pill box – Cellular connectivity • Lights up and beeps when a dose is due • Central database records adherence • Missed doses trigger calls, texts, email • Social involvement (MD, caregiver, etc)
 Med. Minder www. medminder. com • Cost – No upfront costs – $39. 99 per month (base unit) – $44. 99 per month (base unit with med alert) – $64. 95 per month (deluxe lockable unit) • Results? – Customer testimonials only
Med. Minder www. medminder. com • Cost – No upfront costs – $39. 99 per month (base unit) – $44. 99 per month (base unit with med alert) – $64. 95 per month (deluxe lockable unit) • Results? – Customer testimonials only
 Cerepak www. meadwestvaco. com • RFID chip and sensor – Records when pills are punched out – Transmits data to CPU and uploads to centralized database • • Reminders: lights up, plays sounds, and vibrates Has buttons for patient responses or questions Marked towards clinical trials and industry Cost: $75 per package; $250 for reader
Cerepak www. meadwestvaco. com • RFID chip and sensor – Records when pills are punched out – Transmits data to CPU and uploads to centralized database • • Reminders: lights up, plays sounds, and vibrates Has buttons for patient responses or questions Marked towards clinical trials and industry Cost: $75 per package; $250 for reader
 Technologies for the Visually Impaired • Scrip. Talk – RFID Rx adhesive tag – Pharmacy programs label – When placed on the base • Reads – – – Drug Strength Dose Frequency Warnings/precautions www. envisionamerica. com
Technologies for the Visually Impaired • Scrip. Talk – RFID Rx adhesive tag – Pharmacy programs label – When placed on the base • Reads – – – Drug Strength Dose Frequency Warnings/precautions www. envisionamerica. com
 Technologies for the Visually Impaired • Scrip. View – Large “flagged” Rx label – Booklet-style – Large print – 2 D barcode (QR code) • Audible instructions via smartphone – Elderly/low vision patients www. envisionamerica. com
Technologies for the Visually Impaired • Scrip. View – Large “flagged” Rx label – Booklet-style – Large print – 2 D barcode (QR code) • Audible instructions via smartphone – Elderly/low vision patients www. envisionamerica. com
 Technologies for the Visually Impaired • BRL – Braille Rx labels – Embossed Rx data – Clear adhesive applied over the Rx label – Rx verification friendly for pharmacists
Technologies for the Visually Impaired • BRL – Braille Rx labels – Embossed Rx data – Clear adhesive applied over the Rx label – Rx verification friendly for pharmacists
 Future Adherence Technologies
Future Adherence Technologies
 Future Technologies • Proteus Biomedical – – Recently FDA approved Ingestible chip Battery activates when swallowed Uses human conductivity to transmit RFID ingestion signal to skin sensor worn by patient – Sensor forwards ingestions data to mobile device – Mobile device forwards to central adherence database
Future Technologies • Proteus Biomedical – – Recently FDA approved Ingestible chip Battery activates when swallowed Uses human conductivity to transmit RFID ingestion signal to skin sensor worn by patient – Sensor forwards ingestions data to mobile device – Mobile device forwards to central adherence database
 Future Technologies • Magne. Trace – Not FDA approved – Magnet attached to medication – Electromagnetic sensors record when the pill is ingested – Transmits data to mobile device and central database – Also reminds patients of missed doses
Future Technologies • Magne. Trace – Not FDA approved – Magnet attached to medication – Electromagnetic sensors record when the pill is ingested – Transmits data to mobile device and central database – Also reminds patients of missed doses
 Other Available and Future Technologies • Pill Pets -- electronic dog that reminds you to take your meds • e. CAP – RFID pill bottle cap • Tatteltale Pill – alerts caregivers when you miss a dose
Other Available and Future Technologies • Pill Pets -- electronic dog that reminds you to take your meds • e. CAP – RFID pill bottle cap • Tatteltale Pill – alerts caregivers when you miss a dose
 Adherence Conclusions • Patient education is still the most effective method • Physical tools (pillboxes) do improve adherence • Passive electronic technologies MAY improve adherence • Pill ingestion technologies are the “Holy grail” • Multi-faceted approach is a MUST • Customize to the patient
Adherence Conclusions • Patient education is still the most effective method • Physical tools (pillboxes) do improve adherence • Passive electronic technologies MAY improve adherence • Pill ingestion technologies are the “Holy grail” • Multi-faceted approach is a MUST • Customize to the patient
 References 1. 2. 3. 4. 5. 6. 7. 8. AHRQ Health Literacy Universal Precautions Toolkit www. ahrq. gov Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41 Dayer, L. , Heldenbrand, S. , Anderson, P. , Gubbins, P. O. , & Martin, B. C. (2013). Smartphone medication adherence apps: potential benefits to patients and providers. Journal of the American Pharmacists Association, 53(2), 172 -181. Park B, Liver Transplant Handbook; A Guide for your healthcare after liver transplant; www. itns. org www. medactionplan. com www. envisionamerica. com www. medisafeproject. com May, M. (2010). Aiding adherence: five approaches to following prescriptions. Nature Medicine, 16(5), 504 -504.
References 1. 2. 3. 4. 5. 6. 7. 8. AHRQ Health Literacy Universal Precautions Toolkit www. ahrq. gov Fine RN, et al. Nonadherence Consensus Conference Summary Report; American Journal of Transplantation 2009; 9: 35– 41 Dayer, L. , Heldenbrand, S. , Anderson, P. , Gubbins, P. O. , & Martin, B. C. (2013). Smartphone medication adherence apps: potential benefits to patients and providers. Journal of the American Pharmacists Association, 53(2), 172 -181. Park B, Liver Transplant Handbook; A Guide for your healthcare after liver transplant; www. itns. org www. medactionplan. com www. envisionamerica. com www. medisafeproject. com May, M. (2010). Aiding adherence: five approaches to following prescriptions. Nature Medicine, 16(5), 504 -504.
 Thank you!
Thank you!
 Questions?
Questions?