f183e2333d12ba066ef42b544bcbb889.ppt
- Количество слайдов: 53



Acute Stroke basics Joshua Z Willey MD MS jzw 2@columbia. edu July 2015

Disclosure Information Relationship with companies who manufacture products used in the treatment of the subjects under discussion Yes____ No __x__ If "Yes, " list company(ies) with the relationship(s) below. Relationship Research Support Manufacturer(s) __ NIH/NINDS: K 23 NS 073104_ Trials: Astrazeneca, Genentech___ Speaker's Bureau ___None_____________ Consultant ___Heartware incorporated___________ Share Holder ___None____________ Other Financial Support __Honoraria from American College of Physicians for MKSAP 17___ Large Gift(s) ____None______________ Relationships with any of the commercial supporters of this CME activity: N/A Discussion of unlabeled uses: Yes _x____ No_____ -Use of intra-arterial t. PA for acute stroke -Discussion on novel anticoagulants for atrial fibrillation

Outline Goals of the hospitalization n Acute stroke treatment n Neurological complications n Medical complications n Secondary prevention n

Why do we hospitalize? n Goals Diagnose stroke subtype n Acute stroke treatment n Secondary stroke prevention n Prevention of medical complications n Prevention of neurological complications n Initiation of rehabilitation n

Question n Which of the following interventions reduces the risk of death and dependency at one year after ischemic stroke? A. Statins n B. DVT prophylaxis n C. Admission to a stroke unit n D. Administration of t. PA n

Question n Which of the following interventions reduces the risk of death and dependency at one year after ischemic stroke? n C. Admission to a stroke unit

Stroke Unit n n Admission to a stroke unit reduced mortality at one year, and improves clinical outcomes Stroke unit: “a term used to describe the focusing of care for stroke patients in hospital under a multidisciplinary team who specialize in stroke management” n n n A discrete ward is better, and no change in length of stay Use of guidelines for dysphagia, DVT prophylaxis Adherence to nursing protocols, including early discontinuation of Foley catheters Early rehabilitation Organization of multi-disciplinary team, presence of specialists across multiple disciplines, and education Cochrane database syst rev 2007

Requirements for certification Continuous QA process n 24/7 neurology coverage n Neurosurgery back up n Stroke unit n Documentation n Dysphagia screening n NIHSS n t. PA administration, including reasons why it was not administered n

Why do stroke units work? Specialized nursing n Emphasis on dysphagia protocols n Early mobilization and rehabilitation n Early discontinuation of Foley catheters n Multi-disciplinary care n DVT prophylaxis protocols n

Diagnostic Testing n n Stroke is primarily a clinical diagnosis CT of head without contrast n Clinical exam alone cannot distinguish ICH from ischemic (Runchey, JAMA 2010) n n MRI without contrast Vascular Imaging n n MRA: tends to overcall stenosis CTA: calcifications and contrast load Doppler: gives only a range, measures actual flow Acute Stroke Tests: CBC, Coags, BMP, Troponin, EKG, CXR

The Stroke-focused Neuro Exam The NIHSS 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Level of consciousness Gaze Maximum Score Visual fields = 42 Facial strength Arm strength Leg strength Limb ataxia (FNF, heel-down-shin) Sensation (pinch / pinprick) Language (re: aphasia) Dysarthria Extinction / inattention (bilateral sensory) For further details see http: //www. americanheart. org

CT Head Without Contrast n Initial test of choice for all acute strokes High sensitivity for ICH n Early infarct signs: dense MCA sign, loss of the insular ribbon, sulcal effacement n Obvious evidence of infarction should lead to rethinking the time of onset. Usually CT not obvious until 24 hours n Poor sensitivity even several days after onset for brainstem or small infarcts n

Loss of the Insular ribbon Sulcal effacement Normal Dense MCA sign

Nl = 10 pts Figure 1. ASPECTS study form A=anterior circulation; P=posterior circulation; C=caudate; L=lentiform; IC=internal capsule; l=insular ribbon; MCA=middle cerebral artery; Ml=anterior MCA cortex; M 2=MCA cortex lateral to insular ribbon; M 3=posterior MCA cortex; M 4, M 5, and M 6 are anterior, lateral, and posterior MCA territories immediately superior to Ml, M 2, and M 3, rostral to basal ganglia. Subcortical structures are allotted 3 points (C, L, and 1 C). MCA cortex is allotted 7 points (insular cortex, Ml, M 2, M 3, M 4, M 5, and M 6). Barber, Lancet 2000

Vascular Imaging n MRA n n Tends to over-estimate stenosis, and prone to artifact. MRA of the neck without contrast is NOT sufficient for recommending CEA Contrast MRA provides better resolution, and allows visualization of the aortic arch and VA origins CTA / CTP n n Used increasingly in acute stroke as initial diagnostic test – when this is done inc in DTN Provides good estimate of degrees of stenosis, especially in the carotids, though calcifications can make interpretation difficult

Vascular Imaging n Doppler: actual measure of flow n n n Digital subtraction angiography n n n Duplex used for carotid artery studies: useful screening test, but sensitivity and specificity may be less than other modalities (Latchaw, Stroke 2009) TCD allows for detecting stenosis and occlusion Gold standard for measuring degrees of stenosis Potential therapeutic value For carotid intervention, CTA or MRA with contrast have the greatest sensitivity and specificity (Latchaw, Stroke 2009)

Other Diagnostic Tests n Laboratory n n Echocardiography n n n Lipid Panel Hg. A 1 c Hypercoagulable Testing (case-by-case basis) Controversy over TTE and/or TEE may have a yield as high as 11%, though PFO is often included Cardiac CTA may be a reasonable alternative Telemetry n n In house yield of 4. 6% (Liao, Stroke 2007) Outpatient: prolonged cardiac monitoring for 21 days in cryptogenic stroke yield of 25 -33% (Tayal, Neurology 2008)

Acute Management of Stroke n Only FDA-approved treatment for acute ischemic stroke remains IV t. PA Proven as clinically efficacious in the NINDS t. PA trials. Outcome was NOT at 24 hours, but rather at 3 months n Main complication is hemorrhage, intra-cranial or extra-cranial n n Few get it or have access to it (Kleindorfer, Stroke 2009) 64% of hospitals do not give t. PA n 40% of the population lives in counties where < 3% get t. PA n

Acute Ischemic Stroke: Contraindications to t. PA n n n n Minor symptoms or rapidly improving Seizure at onset Other stroke or trauma within 3 months Major surgery in the last 14 days Known hx of ICH Sustained BP > 185/110 Aggressive Rx needed to control BP n n n n NINDS t. PA trial. NEJM 1995 Suspicion for SAH GI or GU hemorrhage in the last 21 days Arterial puncture at a noncompressible site within 7 days Received heparin within the last 48 hours and PTT elevated INR > 1. 7 Platelet count < 100, 000 Glucose < 50 or > 400

Contraindications: 2013 Significant head trauma or prior stroke in 3 months SAH Noncompressible arterial puncture Intracranial pathology Recent neurosurgery Elevated BP Acute bleeding risk (platelet count, a. PTT, INR, novel anticoagulant) Glucose < 50 mg/dl > 1/3 cerebral infarct RELATIVE: Too good to treat Pregnancy Seizure at onset Major surgery or trauma within 14 days Recent GI/GU bleed Recent acute MI

New thrombolysis statement: 2016 n n n n Pediatric use not well established Age is not an exclusion Severe strokes t. PA indicated Mild and disabling strokes: t. PA indicated Mild and non-disabling: less certain Potential harm in intra-axial malignancy Stroke mimics and prior ASA n n n Demaerschalk, Stroke 2016 t. PA not indicated if INR > 1. 7 or LMWH NOAC’s: Normal labs or missed doses for 48 hours Can treat most cardiac patients Safe with cerebral microbleeds, harmful if ICH history Can be considered with endstage medical illness Giving antiplatelets not safe

What’s new in guidelines? Do not need labs n Can treat if recent GI/GU bleed and non-major surgery n Novel anticoagulants n Recent neurosurgery, other surgery may be considered n Seizure at onset, too good to treat n Adapted from Stroke 2015

Meta-analysis of rt-PA-based Thrombolytic Trials NINDS, ATLANTIS, & ECASS TRIALS Lancet 2004; 363: 768 -74.
 Placebo (%) Symptomatic hemorrhage (36 hrs)")
TPA for Acute Stroke: Associated Risks TPA (%) Placebo (%) Symptomatic hemorrhage (36 hrs) 6. 4 (50% of these died) 0. 6 Asymptomatic hemorrhage (36 hrs) 4. 5 2. 9 Neurologic deterioration from all causes (24 hrs) 17. 4 18. 3 Mortality (3 mos) 17. 0 20. 0 NEJM 1995; 333: 1581 -7; Haley et al. Ann Emerg Med 1997; 30: 676 -82.

HI-1 PH-1 ECASS hemorrhagic transformation grading scheme HI-2 PH-2 Only PH-2 has been associated with poor neurological outcomes

Problems with IV t. PA n Hemorrhage Risk factors: early CT changes, hyperglycemia, HTN, size of infarct on DWI, protocol violation n Other : anti-platelet agents, cerebral microbleeds, statins, age, disruption of the blood brain barrier, hemodynamic failure n Reocclusion after recanalization (34%) n Failure to recanalize (depends on vessel) n n n ICA T >> M 1 >> M 2 Angioedema (~ 2%) The NICU book CH 5
 n Benefit of IV")
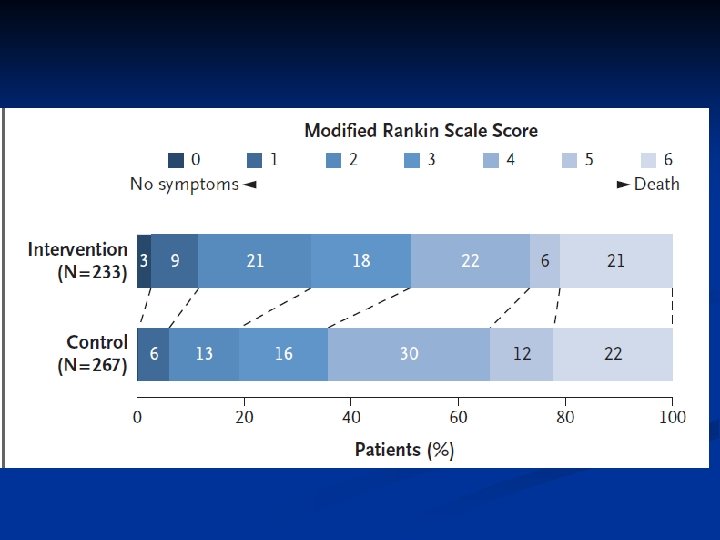
Treatment Beyond 3 Hours n ECASS III (Hacke, NEJM 2008) n Benefit of IV t. PA up to 4. 5 hours from onset, in a highly selected group of patients n 52. 4% vs. 45. 2 % achieved favorable outcome (m. RS 0 -1) – OR 1. 35, 1. 02 -1. 76 n IST-3 (Lancet 2012) brings into question treatment up to 6 hrs, but established use for those over 80

Treatment Beyond 3 Hours n Intra-arterial treatment formerly indicated for a major vessel occlusion if no TPA 3 -6 hours Intra-arterial thrombolytic studied in the PROACT study (JAMA 1999). Clinical benefits at 3 months. n 3 clinical trials failed to show a benefit of endovascular therapy after IV t. PA (IMS III, NEJM 2013), compared to IV TPA (SYNTHESIS, NEJM 2013), or based on multi-modality imaging (MR Rescue, NEJM 2013) n

Treatment beyond 3 hours n Why did they not work n n MR CLEAN (NEJM 2014): all outcomes favored INR treatment - ~ 90% t. PA before n n No CTA, no modern stent retrievers Inclusion: intracranial occlusion, NIHSS 2 or more Baseline: ASPECTS 9, most non-disabled, 85% M 1 and ICA T occlusions, ~ 180 minutes to INR m. RS 4 vs 3, 0 -2 in 33 vs 19 percent, 8 vs 14 NIHSS at 5 days, 30 cc smaller infarct Similar results in EXTEND-IA, ESCAPE, SWIFTPRIME (all 2015)

Acute Stroke: Medical Treatment n Acute anti-platelet agents n CAST, Lancet 1997: ASA 160 mg vs. placebo for 4 weeks. n ARR from 3. 9 to 3. 3 % in early mortality, and repeat stroke from 2. 1 to 1. 6% n IST, Lancet 1997: ASA 300 mg vs. none, and sq heparin 5000 vs. 12500 bid. n At 14 days there were NS fewer deaths in the ASA group (9% vs 9. 4 %), with fewer strokes (2. 8% vs 3. 9%), with no increase in ICH.
. 24 hours of minor")
Medical treatment n FASTER trial ( (Kennedy, Lancet Neurol 2007). 24 hours of minor stroke/TIA to clopidogrel (300 mg load, 75 mg daily) versus placebo. All on ASA n n CHANCE (NEJM 2013): ASA / clopidogrel x 21 days followed by clopidogrel within 24 hrs– reduced risk of stroke at 90 days, trial in China n n Trial stopped early due to slow recruitment At 90 days 7. 1% vs 10. 8% had a recurrence 10. 6% vs 7. 3% for recurrence in statin vs placebo (p = 0. 25) ARR: 8. 2% vs 11. 7%, no difference in bleeding Ticagrelor not effective vs ASA (NEJM 2016)

Heparin in Acute Stroke n n n Negative clinical trial of heparin in acute cardio-embolic stroke from A-fib (Berge, Lancet 2000) TOAST for all non-cardioembolic strokes also negative Eminence based medicine: IV heparin in acute carotid dissection? Frequently used in the setting of a mechanical valve If the stroke is small, can also be considered in postoperative atrial fibrillation

Ischemic Stroke: Hypertension n In IV TPA eligible patients: Pretreatment < 185/110, post < 180/105 n IV labetalol or nicardipine n n In IV TPA ineligible patients with ischemic stroke: Goal < 220/120 until hospital discharge unless there is evidence of end organ damage (MI, CHF) n We tend to not hold diuretics and beta blockers n n No clinical efficacy from early BP lowering and a trend towards worse neurological outcomes (SCAST, Lancet 2011)

Other Acute Stroke Management n Hemorrhagic stroke No agents have proven to be effective in the acute setting, including factor VII (Mayer, NEJM 2008) n Lowering BP to SBP 140 if starting 150 -220; target not much lower (Qureshi, NEJM 2016) n No clear evidence to support platelet transfusions n PCC preferred over FFP – need vitamin K n Surgery can be considered in non-cerebellar ICH near cortical surface… n DVT prophylaxis sooner than later n Stroke 2015

Statin agents n n Consistent primary prevention role SPARCL, NEJM 2008: n n n ~4731 patients with an LDL > 100 and stroke/TIA randomized to atorvastatin 80 mg vs placebo. Achieved ~ 50 mg/dl difference in LDL. Outcome: fatal or non-fatal stroke Ischemic stroke regardless of lipid levels (13. 1% vs 11. 2%) Increase in ICH (HR 1. 66); 2. 2% vs 0. 5% inc ni LFT’s, no liver failure or rhabdomyolysis No phase III trials of statins in acute stroke! n Statins should be avoided in ICH, esp lobar n Arch Neurol 2011) (Westover,
. (Fiorelli M, Stroke 2001) n")
Neurologic Complications of Stroke n Hemorrhagic conversion (~36 hours). (Fiorelli M, Stroke 2001) n n RF of HC: large infarct, cardio-embolic, elevated glucose, thrombolytic (Stroke 2008; 39: 2249) Mass effect and cerebral edema. Occurs in up to 10% and peaks at day 2 -5 (Vahedi K, Lancet Neurol 2007). n RF: high NIHSS, > 50% MCA infarction, early N/V (Stroke 2001) Recurrent stroke (rare) n Seizures: more common with hemorrhagic stroke n INFECTION/Toxic metabolic n

42 year man with hypertension and tobacco use presents to your office for 10 minutes of left arm clumsiness. His medications include aspirin and HCTZ. His examination is normal. What is the most appropriate next step in management? n A. Obtain an MRI brain n B. Start warfarin n C. Change to clopidogrel n D. Carotid ultrasound n E. Check echocardiogram

42 year man with hypertension and tobacco use presents to your office for 10 minutes of left arm clumsiness. His medications include aspirin and HCTZ. His examination is normal. What is the most appropriate next step in management? n D. Carotid ultrasound

Short-term Prognosis After ED Diagnosis of TIA 30. 0% 25. 0% Outcome events • N=1707 • Inclusion criteria: TIA by ED 20. 0% • Short-term risk (90 days) 15. 0% 10. 0% 5. 0% 0. 0% 12. 7% • Total risk 25% 10. 5% Within 90 days 5. 3% 2. 6% Within 48 hr Stroke Recurrent TIA 2. 6% CV event Death Johnston SC, et al. JAMA 2000; 284: 2901 -6.

ABCD 2 Score SCORE FACTORS 1 Age ≥ 60 years 1 Blood pressure ≥ 140/90 mm. Hg on first evaluation 2 Clinical symptoms of focal weakness with the spell (or) speech impairment without weakness 1 2 1 Duration ≥ 60 minutes (or) 10 to 59 minutes 1 Not a TIA diagnostic tool! Diabetes AHA / ASA 2009 Recommended admission for all patients with an ABCD 2 ≥ 3 ABCD 2 SCORE 2 DAY STROKE RISK 0– 1 0% 2– 3 1. 3% 4– 5 4. 1% 6– 7 8. 1%

Internal carotid artery disease n Carotid Endarterectomy for Symptomatic disease > 70% (NASCET, NEJM 1991). n n CREST (NEJM 2010). CEA CAS are overall equivalent n n Clear benefit for CEA versus maximal medical treatment. 13% per year vs. 5% in the surgical arm (NNT 17). The earlier the better! (1% per day risk of stroke in first 2 weeks) (Rothwell, Neurology 2005). Symptomatic disease 50 -79%: more modest benefit (6. 5% absolute benefit in 5 years) CEA is associated with a lower risk of immediate and delayed stroke, but an increased risk of MI ICSS (Lancet 2010) showed better outcomes with CEA

Our patient: 2 ABCD =2
 (Kumar, Lancet Neurol 2010) PE/DVT")
Medical complications after stroke n Acute complications (24 -95%) (Kumar, Lancet Neurol 2010) PE/DVT (0. 2 -4%) n Falls (2. 2 -25%) n UTI (6. 3 -30. 5%) n PNA (4 -22%) n MI (0. 5 -4%) n CHF (2 -11%) n n Stroke is a coronary heart disease equivalent (Dhamoon, n Sleep-related breathing and sleep-wake disturbances n Other chronic complications: depression, bed sores, incontinence, pain, fatigue Circulation 2010) (Hermann, Neurology 2009)

Infectious complications n Pneumonia is one of the most common stroke complications, and main cause of fever within 48 hrs. Associated with 3 x inc mortality n n n Difficult to distinguish PNA from aspiration pneumonitis RF: age, speech disturbance, severity of stroke, dysphagia Dysphagia (11 x inc risk of PNA) – SCREEN! DT and PEG do not actually reduce incidence Oral care and dental hygeine may help UTI n n Urinary dysfunction very common after stroke, but UTI most likely due to prolonged Foley catheter use Not as strongly associated with poor outcomes

Cardiovascular complications n n Most cardiac complications occur early in the hospital course, esp in history of CHF, DM, severe stroke, CRI, and inc QTc (Prosser Stroke 2007) Acute MI: elevated troponins after stroke common (0. 56%) n n Congestive heart failure: affects mortality n n n Myocytolysis/neurogenic troponins: R insular infarcts, large stroke and hemorrhage. Levels cannot help distinguish these from cardiac induced Many patients with stroke also have silent CAD, esp those with large artery athero New onset: MI, arrhythmia, HTN, Takatsubo Exacerbation: iatrogenic Cardiac arrythmias

Pulmonary complications n n n Hypoxemia: sleep apnea, PNA, PE, atelectasis. Associated with mortality, and more likely in patients with known CP dz Oxygen trial so far negative DVT and PE: most occur within the week n n n Risk factors for DVT: age, paralysis, and dehydration DVT prophylaxis: LMWH appears to be superior to SQ heparin Recommend to start day 1 -4 after bleeding is no longer active in ICH Sequential compression devices are effective, while graduated compression stockings are not Suspect in delayed hypoxemia, especially when DVT prophylaxis has been held Sleep disordered breathing commonly observed in the acute setting. Age, severity, dec EF inc the risk. Kumar, Lancet Neurol 2009

GI complications n Dysphagia: 37 -78% of patients n n n Besides PNA, inc risk of malnutrition and dehydration PEG and DT do not prevent PNA. PEG is more effective long tern than DT/NGT FOOD trial (Dennis MS, Lancet 2005). Trial stopped early due to poor funding so underpowered. No overall advantage to early feeding, with a trend to benefit. n n PEG associated with borderline significant inc in death or poor outcome Authors concluded that early PEG may not be warranted Oral hygeine reduces PNA GI bleed rare, but occurs in same patients that can get stress ulcers. Prophylaxis can inc the risk of PNA

Psychiatric and others n Post stroke depression n n n Present in up to 25% of stroke patients, observed within one week and peaks at 3 months (Robinson, Biol Psych 2003) Significantly affects functional recovery (Willey, Stroke 2010) Treatment for depression improves outcomes, especially when psychotherapy and medications are combined (Robinson JAMA 2008). Cochrane database review 2008: no good treatment for prevention or abatement of depression Falls and bed sores Medication adherence associated with decreasing numbers of medications, inc age, medical history, less severe disability, having insurance and working, understanding why medications are prescribed, and financial hardship (Bushnell, Arch Neurol 2010)
: 2206 with noncardioembolic stroke were")
Warfarin Without Atrial Fibrillation WARSS (Mohr JP, NEJM 2001): 2206 with noncardioembolic stroke were randomized to warfarin (INR 1. 4 -2. 8) vs. ASA 325 mg. Mean INR 2. 1. No difference in effectiveness or safety. n WASID (Chimowitz MI, NEJM 2005): 569 pts with symptomatic intracranial atherosclerosis were randomized to ASA 1300 mg vs. warfarin daily. Trial stopped early by DSMB due to excess events (death, MI, hemorrhage) in warfarin group. n

AF: Medical treatment Robust clinical benefit and safety of warfarin for atrial fibrillation in several trials n Dabigatran (direct thrombin inhibitor) (Connolly SJ; NEJM n 2009) n n Warfarin 1. 69%/yr stroke systemic embolism, 1. 53% for 110 mg (p< 0. 001 noninferior), 1. 11% for 150 mg (p < 0. 001 superior). Lower rates of major hemorrhage with dabigatran (3. 36%, 2. 71%, 3. 11%) Rivaroxaban (direct factor Xa inhibitor) vs. warfarin non-inferiority trial. Outcome occurred in 1. 7%/yr verus 2. 2%/yr with a slightly better safety profile (Patel, NEJM 2011)

Conclusions n The goals of hospitalization are: Identification of stroke type n Prevention of immediate neurological complications n Prevention of medical complications n n Medical complications overwhelmingly affect stroke related mortality and recovery n Many of these complications are preventable, likely through admissions to stroke units
f183e2333d12ba066ef42b544bcbb889.ppt