

f5704ec8457f61838cbaf170e0880777.ppt
- Количество слайдов: 33
 Acute Renal Failure Terry Cook Imperial College London
Acute Renal Failure Terry Cook Imperial College London
 Acute Renal Failure • Rapid loss of glomerular filtration and tubular function leading to abnormal water, electrolyte and solute balance • Occurs over hours to days • Usually associated with oliguria. Some patients develop non-oliguric ARF eg. After radiocontrast media • Acute-on chronic renal failure
Acute Renal Failure • Rapid loss of glomerular filtration and tubular function leading to abnormal water, electrolyte and solute balance • Occurs over hours to days • Usually associated with oliguria. Some patients develop non-oliguric ARF eg. After radiocontrast media • Acute-on chronic renal failure
 Aetiology of ARF • Pre-renal • Renal – Glomerular – Tubulointerstitial – Vascular • Post-renal
Aetiology of ARF • Pre-renal • Renal – Glomerular – Tubulointerstitial – Vascular • Post-renal
 Aetiology of ARF • Glomerular – RPGN • Tubulointerstitial – – Acute tubular necrosis Acute tubulointerstitial nephritis Infection Cast nephropathy • Vascular – Thrombotic microangiopathy – Cholesterol emboli – Vasculitis
Aetiology of ARF • Glomerular – RPGN • Tubulointerstitial – – Acute tubular necrosis Acute tubulointerstitial nephritis Infection Cast nephropathy • Vascular – Thrombotic microangiopathy – Cholesterol emboli – Vasculitis
 • RPGN is a clinical term for clinical manifestations that") Rapidly Progressive Glomerulonephritis (RPGN) • RPGN is a clinical term for clinical manifestations that suggest severe crescentic glomerulonephritis • Crescentic glomerulonephritis – may be used for glomerulonephritis with any crescents but WHO suggests >50%
Rapidly Progressive Glomerulonephritis (RPGN) • RPGN is a clinical term for clinical manifestations that suggest severe crescentic glomerulonephritis • Crescentic glomerulonephritis – may be used for glomerulonephritis with any crescents but WHO suggests >50%
 Crescentic glomerulonephritis • Crescents are an indication of severity of glomerulonephritis rather than its cause • Complete pathological diagnosis requires analysis of immunofluorescence, electron microscopy and serology
Crescentic glomerulonephritis • Crescents are an indication of severity of glomerulonephritis rather than its cause • Complete pathological diagnosis requires analysis of immunofluorescence, electron microscopy and serology
 Natural history of crescents Breach in integrity of GBM – ROS, proteases etc from inflammatory cells Cells and fibrin in Bowman’s space Accumulation of macrophages and proliferating epithelial cells Apoptosis of cells and laying down of collagen Fibrocellular crescents and fibrous crescents
Natural history of crescents Breach in integrity of GBM – ROS, proteases etc from inflammatory cells Cells and fibrin in Bowman’s space Accumulation of macrophages and proliferating epithelial cells Apoptosis of cells and laying down of collagen Fibrocellular crescents and fibrous crescents
 Causes of crescentic glomerulonephritis • Anti-GBM disease • Immune complex disease • Pauci-immune
Causes of crescentic glomerulonephritis • Anti-GBM disease • Immune complex disease • Pauci-immune
 Frequency of types of crescentic GN Any Crescents >50% crescents Arteritis in Biopsy Anti-GBM 5% 11% 3% Immune complex 49% 29% 14% Pauciimmune 47% 61% 84% After Jenette and Falk
Frequency of types of crescentic GN Any Crescents >50% crescents Arteritis in Biopsy Anti-GBM 5% 11% 3% Immune complex 49% 29% 14% Pauciimmune 47% 61% 84% After Jenette and Falk
 10 -19 20 -39 40 -64") Frequency of types of crescentic GN Age (years) 10 -19 20 -39 40 -64 >65 Anti-GBM 15% 24% 2% 11% Immune complex 50% 48% 30% 8% Pauciimmune 35% 28% 69% 82%
Frequency of types of crescentic GN Age (years) 10 -19 20 -39 40 -64 >65 Anti-GBM 15% 24% 2% 11% Immune complex 50% 48% 30% 8% Pauciimmune 35% 28% 69% 82%
 Crescent formation in different glomerular diseases Patients with any crescents Patients with >50% crescents Anti-GBM disease 95 81 Pauci-immune (ANCA-associated) 90 48 Lupus GN (class III and IV) 40 11 Henoch-Schonlein purpura 53 5 Ig. A nephropathy 27 5 Postinfectious GN 25 3 Fibrillary GN 20 7 Type I membranoproliferative GN 20 3
Crescent formation in different glomerular diseases Patients with any crescents Patients with >50% crescents Anti-GBM disease 95 81 Pauci-immune (ANCA-associated) 90 48 Lupus GN (class III and IV) 40 11 Henoch-Schonlein purpura 53 5 Ig. A nephropathy 27 5 Postinfectious GN 25 3 Fibrillary GN 20 7 Type I membranoproliferative GN 20 3
 Crescentic GN – Differential diagnosis Light microscopy Immunofluorescence Other Anti-GBM Synchronous crescents Linear Ig. G and C 3 Circulating anti. GBM antibody Pauci-immune Focal and segmental necrosis +/- vasculitis Scanty ANCA Immune complex Focal and segmental or global hypercellularity Various e. g lupus serology, cryoglobulins etc
Crescentic GN – Differential diagnosis Light microscopy Immunofluorescence Other Anti-GBM Synchronous crescents Linear Ig. G and C 3 Circulating anti. GBM antibody Pauci-immune Focal and segmental necrosis +/- vasculitis Scanty ANCA Immune complex Focal and segmental or global hypercellularity Various e. g lupus serology, cryoglobulins etc
 Anti-GBM disease • • • Presents with RPGN often accompanied by lung haemorrhage Rare disorder (1 pmp) predominantly in Caucasian populations Characterised by circulating and deposited anti-GBM antibodies
Anti-GBM disease • • • Presents with RPGN often accompanied by lung haemorrhage Rare disorder (1 pmp) predominantly in Caucasian populations Characterised by circulating and deposited anti-GBM antibodies
 Immune complex crescentic GN Immunofluorescence Electron microscopy Clinical Lupus WHO Class III or IV “Full House” Deposits at all sites Tubulo-reticular bodies Serology, anti-C 1 q etc Henoch Schonlein purpura Ig. A, C 3 Mesangial +/- capillary wall deposits Rash, arthralgia, abdominal pain Ig. A nephropathy Ig. A, C 3 Mesangial +/- capillary wall deposits History of sore throat Membranoproliferative GN Type I Capillary wall C 3 +/others Subendothelial deposits Double contours Infections eg. Hep C Cryoglobulins Post-infectious GN Capillary wall C 3 +/Ig. G “humps” ASOT Fibrillary GN Mesangial Ig. G, C 3 Fibrils
Immune complex crescentic GN Immunofluorescence Electron microscopy Clinical Lupus WHO Class III or IV “Full House” Deposits at all sites Tubulo-reticular bodies Serology, anti-C 1 q etc Henoch Schonlein purpura Ig. A, C 3 Mesangial +/- capillary wall deposits Rash, arthralgia, abdominal pain Ig. A nephropathy Ig. A, C 3 Mesangial +/- capillary wall deposits History of sore throat Membranoproliferative GN Type I Capillary wall C 3 +/others Subendothelial deposits Double contours Infections eg. Hep C Cryoglobulins Post-infectious GN Capillary wall C 3 +/Ig. G “humps” ASOT Fibrillary GN Mesangial Ig. G, C 3 Fibrils
 Pauci-immune crescentic GN • Basic lesion is focal and segmental necrosis • Often associated with vasculitis either in kidney or elsewhere
Pauci-immune crescentic GN • Basic lesion is focal and segmental necrosis • Often associated with vasculitis either in kidney or elsewhere
 Pauci-immune crescentic GN syndromes 1. 2. 3. 4. Limited to kidney Microscopic polyangiitis – necrotizing vasculitis in other systems including skin, mucous membranes, lungs, brain, gastrointestinal tract and muscle Wegener’s granulomatosis – similar lesions to microscopic polyangiitis together with necrotizing granulomas of the upper and lower respiratory tract Churg-Strauss syndrome – history of asthma or allergic rhinitis and blood eosinophilia N. B. These syndromes cannot be distinguished on the basis of renal histology
Pauci-immune crescentic GN syndromes 1. 2. 3. 4. Limited to kidney Microscopic polyangiitis – necrotizing vasculitis in other systems including skin, mucous membranes, lungs, brain, gastrointestinal tract and muscle Wegener’s granulomatosis – similar lesions to microscopic polyangiitis together with necrotizing granulomas of the upper and lower respiratory tract Churg-Strauss syndrome – history of asthma or allergic rhinitis and blood eosinophilia N. B. These syndromes cannot be distinguished on the basis of renal histology
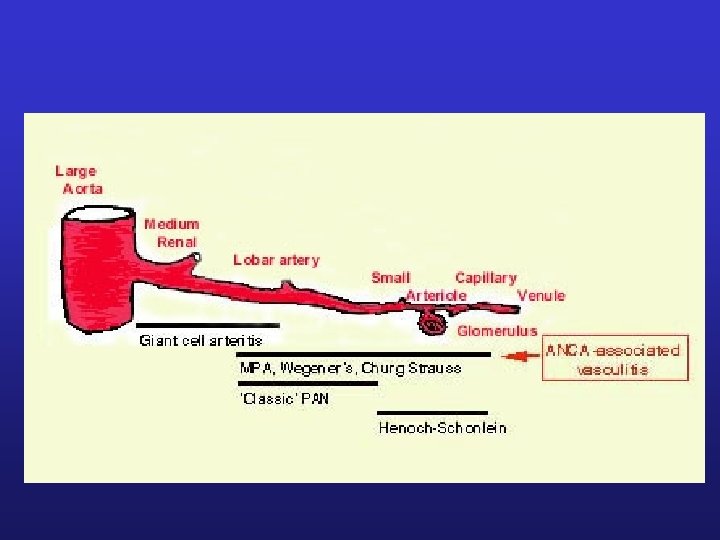
 ANCA in small vessel vasculitis IIF pattern: Antigen: Syndromes: C-ANCA Proteinase 3 WG, MP P-ANCA Myeloperoxidase MP, renal-limited vasculitis
ANCA in small vessel vasculitis IIF pattern: Antigen: Syndromes: C-ANCA Proteinase 3 WG, MP P-ANCA Myeloperoxidase MP, renal-limited vasculitis
 Clinical studies of ANCA • Specific and sensitive marker for systemic vasculitis • ANCA pattern and specificity correlate with clinical features • Levels correlate with disease activity and extent • Rising levels predict relapse
Clinical studies of ANCA • Specific and sensitive marker for systemic vasculitis • ANCA pattern and specificity correlate with clinical features • Levels correlate with disease activity and extent • Rising levels predict relapse
 European Vasculitis Study Group biopsy findings • • Biopsies from 96 patients with ANCAassociated vasculitis and creatinine <500 mmol/l Studied – – – GFR 0 – GFR at presentation GFR 18 – GFR at 18 months CORGFR 18 – GFR at 18 months corrected for GFR 0
European Vasculitis Study Group biopsy findings • • Biopsies from 96 patients with ANCAassociated vasculitis and creatinine <500 mmol/l Studied – – – GFR 0 – GFR at presentation GFR 18 – GFR at 18 months CORGFR 18 – GFR at 18 months corrected for GFR 0
 European Vasculitis Study Group biopsy findings • Predictors for GFR 0 – %normal glomeruli – %glomeruli with crescents – Extent of tubular atrophy and interstitial fibrosis
European Vasculitis Study Group biopsy findings • Predictors for GFR 0 – %normal glomeruli – %glomeruli with crescents – Extent of tubular atrophy and interstitial fibrosis
 European Vasculitis Study Group biopsy findings • Predictors for CORGFR 18 – % glomeruli with fibrinoid necrosis – % glomeruli with cellular crescents – Tubulointerstitial inflammation • Tubular atrophy and interstitial fibrosis did not predict CORGFR 18 even though they correlated with GFR 18 implying that this was dependent on GFR 0
European Vasculitis Study Group biopsy findings • Predictors for CORGFR 18 – % glomeruli with fibrinoid necrosis – % glomeruli with cellular crescents – Tubulointerstitial inflammation • Tubular atrophy and interstitial fibrosis did not predict CORGFR 18 even though they correlated with GFR 18 implying that this was dependent on GFR 0
 European Vasculitis Study Group biopsy findings • In ANCA GN the best histological predictors of long-term renal function are – Normal glomeruli, glomerulosclerosis, interstitial fibrosis and tubular atrophy • The best predictors of the improvement in renal function from 0 to 18 months are – Crescents, fibrinoid necrosis and interstitial inflammation
European Vasculitis Study Group biopsy findings • In ANCA GN the best histological predictors of long-term renal function are – Normal glomeruli, glomerulosclerosis, interstitial fibrosis and tubular atrophy • The best predictors of the improvement in renal function from 0 to 18 months are – Crescents, fibrinoid necrosis and interstitial inflammation
 Acute tubular necrosis • Prolonged hypoperfusion • Drugs – NSAIDs, ACE inhibitors • Direct toxicity – – – Drugs – eg. Aminoglycosides, cisplatin Radiocontrast agents Haem pigments Snake venom Heavy metals – lead , mercury • Associated with nephrotic syndrome
Acute tubular necrosis • Prolonged hypoperfusion • Drugs – NSAIDs, ACE inhibitors • Direct toxicity – – – Drugs – eg. Aminoglycosides, cisplatin Radiocontrast agents Haem pigments Snake venom Heavy metals – lead , mercury • Associated with nephrotic syndrome
 Acute tubular necrosis Tubular dilatation Loss of brush border Epithelial cell vacuolation Detachment of epithelial cells Granular casts Hyperchromasia of tubular nuclei Mitoses Calcification Interstitial oedema Interstitial inflammation Nucleated rbcs in vasa recta
Acute tubular necrosis Tubular dilatation Loss of brush border Epithelial cell vacuolation Detachment of epithelial cells Granular casts Hyperchromasia of tubular nuclei Mitoses Calcification Interstitial oedema Interstitial inflammation Nucleated rbcs in vasa recta
 Acute tubulointerstitial nephritis • • • Infectious eg. HIV, BKV, fungi, TB Drugs Post infectious SLE ANCA associated With uveitis (TINU)
Acute tubulointerstitial nephritis • • • Infectious eg. HIV, BKV, fungi, TB Drugs Post infectious SLE ANCA associated With uveitis (TINU)
 Acute tubulointerstitial nephritis • Interstitial infiltrate of mononuclear cells – Mainly T cells and macrophages • Tubulitis • +/- eosinophils • May rarely be anti-TBM antibodies
Acute tubulointerstitial nephritis • Interstitial infiltrate of mononuclear cells – Mainly T cells and macrophages • Tubulitis • +/- eosinophils • May rarely be anti-TBM antibodies
 Granulomatous tubulointerstitial nephritis • • Infectious Sarcoidosis Drugs Idiopathic
Granulomatous tubulointerstitial nephritis • • Infectious Sarcoidosis Drugs Idiopathic
 Myeloma Cast Nephropathy • Light chains precipitate in tubules • Casts are large and eosinophilic – may be fractured or fragemented • Multinucleate giant cells my be found adjacent to casts • In some cases the casts may stain for amyloid • Interstitium typically shows an infiltrate of lymphocytes and macrophages
Myeloma Cast Nephropathy • Light chains precipitate in tubules • Casts are large and eosinophilic – may be fractured or fragemented • Multinucleate giant cells my be found adjacent to casts • In some cases the casts may stain for amyloid • Interstitium typically shows an infiltrate of lymphocytes and macrophages
 Thrombotic microangiopathy • Haemolytic-uraemic syndrome – – – – Infection – particularly verotoxin-producing E. coli Drugs – CNIs, mitomycin Transplant rejection Antiphospholipid antibodies Post-partum Factor H deficiency Bone marrow transplantation • Thrombotic thrombocytopenic pupura • Malignant Hypertension • Scleroderma
Thrombotic microangiopathy • Haemolytic-uraemic syndrome – – – – Infection – particularly verotoxin-producing E. coli Drugs – CNIs, mitomycin Transplant rejection Antiphospholipid antibodies Post-partum Factor H deficiency Bone marrow transplantation • Thrombotic thrombocytopenic pupura • Malignant Hypertension • Scleroderma
 Thrombotic microangiopathy • Glomeruli – – Thrombosis Trapped fragmented rbc Thickened capillary walls with subendothelial fibrin Ischaemic changes • Arterioles – fibrinoid • Interlobular arteries – loose intimal thickening
Thrombotic microangiopathy • Glomeruli – – Thrombosis Trapped fragmented rbc Thickened capillary walls with subendothelial fibrin Ischaemic changes • Arterioles – fibrinoid • Interlobular arteries – loose intimal thickening
 Cholesterol emboli • Common cause of unexplained renal failure in elderly • Predisposing factors – Trauma eg catheterisation, surgery – Anticoagulation – Spontaneous • May be slowly progressive • May involve glomeruli
Cholesterol emboli • Common cause of unexplained renal failure in elderly • Predisposing factors – Trauma eg catheterisation, surgery – Anticoagulation – Spontaneous • May be slowly progressive • May involve glomeruli