fb708ce27f4df408e0bd2eacf279191d.ppt
- Количество слайдов: 63



ACOEM: Where We Are Headed Karl Auerbach MD, MS, MBA FACOEM President New York Occupational and Environmental Medical Association 10/19/2012

My Goals Today • Remind us that ACOEM is each of us collection of members, components, sections • We are as strong as collective contributions of or members , as volunteers and professionals • Here to listen and learn • Review where ACOEM has been and where we are headed • Foster collaboration

Rounding The Horn “THEN came the cry of "Call hands on deck!" The Dauber knew its meaning; it was come: Cape Horn, that tramples beauty into wreck, And crumples steel and smites the strong man dumb. Down clattered flying kites and staysails; some Sang out in quick, high calls: the fairleads skirled, And from the south-west came the end of the world. . . ” John Masefield

Outline • • Challenges we face How we are organized What have we done What will have to do.

Challenges • • • Recession in western economies Working harder with less Diabesity Aging workforce Health disparities and migrant health Technology and remote work Primary care shortages Healthcare reform We are few in number

Challenges • Occupational medicine physicians are fewer in number. • Occupational medicine physicians are aging. • Training pipeline is pinched. – – Programs Funding Knowledge of field by medical students and residents 132 boarded OM in 2001/74 in 2011

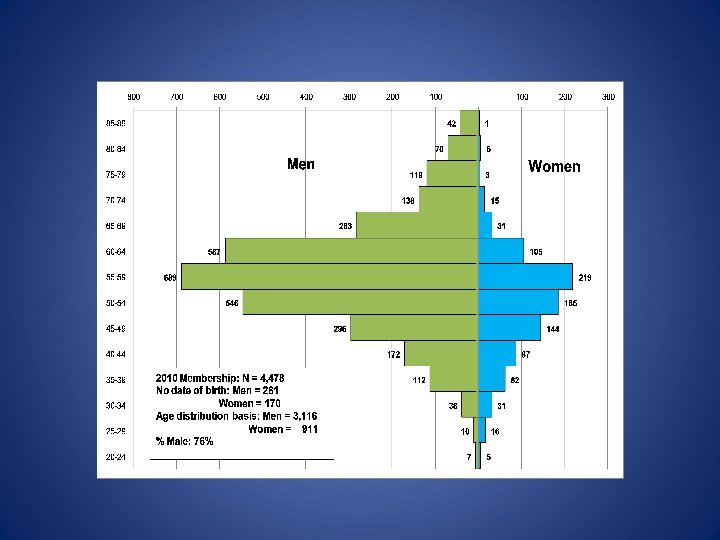
Challenges • ACOEM membership reflects the overall demographic changes. – 6098 in 2001 – 4338 in 2011 – 4397 in 2012 • Yet still robust in getting new members • Issue is mixed but aging a factor

Challenges • Because we are fewer in number but in demand, many of us tend to be as busy or busier than ever. • Doing more with less. • Impact on volunteer activities including ACOEM.

Challenges Primary Care Shortage • “The U. S. will experience a shortage of 35, 000– 44, 000 primary care physicians for adults by 2025. Population growth and aging will increase family physicians’ and general internists’ workloads by 29 percent between 2005 and 2025. “ • [Source: Colwill JM, Cultice JM, Kruse RL. Health Aff (Millwood). 2008 May-Jun; 27(3): w 232 -41. Epub 2008

Challenges • Health care reform will change the way we practice and relate to our patients and organizations. • New models of health care delivery • Claiming the appropriate stake in the new systems.

There are dangers ahead •


What is ACOEM • ACOEM is made up of its members • Organized into components by geography • Organized into sections by interest

Components • 23 Components in the US and Canada – As small as 26 – As large as 551 • Direct membership in many countries • Several component mergers in the last few years.

•

Component Responsibilities Policy and Procedure 2. 01 Responsibility of Components • Components must notify ACOEM Headquarters of any change in component officers within 30 days.

• Component societies must also file a copy of their bylaws with the ACOEM Headquarters Office. Amended bylaws are also to be sent to Headquarters to keep on file. • Components must hold at least 1 business meeting a year that is open to all Component members, and the location of such meetings shall be geographically diverse over a cycle more of no than 3 years so as to maximize potential for attendance by Component members.

• A component must have a fixed mailing address and advise ACOEM of such. The fixed address can be that of an executive director, the office of an appropriate institution (such as a training program), or an officer. • Components must establish and maintain a mechanism necessary to be aware of matters of interest to occupational medicine physicians in the state or states within the Component and bring such matters to the attention of the national organization and the members in a timely fashion.

• Components must submit to ACOEM a written annual report, including a current listing of officers, outlining their activities in the past year. This report will be reviewed by the House of Delegates. • A component is required to have a delegate at each House of Delegates meeting. Those not having a delegate at the ACOEM House of Delegates for at least 1 House Meeting a year will be deemed not to be in compliance with this resolution and the House of Delegates will so advise the Board of Directors.

Sections • Reflect a special interest by topic or industry • 18 Sections • Total section membership: 3, 357 including members in more than one section • Members in at least 1 section: 1, 855 which is about 40% of ACOEM members

Business, Education, Social Networks • Groups of members and others who typically are in a city or region who meet for business, educational or social purposes. • Not part of the ACOEM governance but recognized in ACOEM policy. • Often not known to ACOEM headquarters. • Urged to let ACOEM headquarters know who they are and what they do.
 Associates Affiliates Retired Residents Medical Students")
ACOEM Membership • • • Active (members, fellows) Associates Affiliates Retired Residents Medical Students

Associates and Affiliates • Active Members, Fellows and Masters -physicians • Associates – Non-physicians with a doctorate degree of Ph. D, Sc. D, Dr. PH, or Ed. D in an occupational and environmental health discipline. Mostly academic and research • Affiliates – Non MD practitioners working in OEM – RN, MPH, JD, PA

Associates/Affiliates • Half of components have lower component dues for associates and affiliates • Associate/affiliate dues are not scheduled for increase in 2013 • Affiliates open house at AOHC 2012 in LA – Affiliate attendees were invited to drop in and tell us what activities would be useful for ACOEM to provide for them.

ACOEM Structure • ACOEM Board of Directors elected by the membership at large. • ACOEM Officers elected by the membership at large. • ACOEM Delegates named by Components or Sections • Delegates elect the House Officers

ACOEM Structure • Executive Committee- officers of ACOEM , speaker of HOD and immediate past president; exercise the authority of the BOD in the management of the business of the College between meetings of the BOD

ACOEM Structure • Councils- primary bodies within ACOEM for programs and projects – Education and Academic Affairs – OEM Practice – Public Affairs – Scientific Advisors

ACOEM Structure • Councils have various committees or task forces depending on the need. In theory these are not enduring committees but are designated as need arises.

ACOEM Structure • Committees of the College – Level 1: Board committees • Finance and Audit • Policies, Procedures and Public Positions (4 Ps) • Strategic planning – Level 2: Primarily Board but may include selected non Board members • • Awards Fellowship Examiners House Board Liaison Joint House Board Nominating

ACOEM Structure • Level 3 Committees: open to all ACOEM members – Membership – Bylaws – Ethics – Guideline methodology – Evidence based medicine

ACOEM Structure • College has a limited number of task forces for specific projects. • Task forces dissolve after they have completed work.

ACOEM Structure • Staff includes executive director • Support areas include – Education – Membership – IT – Finance – Guidelines – Development

ACOEM Structure • ACOEM is a mixed volunteer and staff organization. • Staff supports the volunteers • Volunteers support staff • Staff provides member services
 $415 in 2013 (Can save if sign")
ACOEM Membership National Dues Active : (increased) $415 in 2013 (Can save if sign up for auto renewal) Associate: $225 no changes in 2013 Affiliate: $225 no changes in 2013 Resident: $45 no changes in 2013 (residents get incentives to participate) • Medical Student: Free • Retired: $25 ($95 -JOEM) no changes 2013 • • •

ACOEM Sample Highlights • ACOEM Guidelines – 3 rd Edition • Complementary Pathway to ABPM Occupational Medicine Board Certification • ACOEM Washington, D. C. advocacy: NIOSH funding cuts; IOM ERM meeting; ACOEM’s Agenda for Change • White paper on “Health Protection and Promotion” NIOSH/CDC • Partnership – IAIABC/ACOEM – workers’ compensation reform

ACOEM Sample Highlights • Letter to Homeland Security regarding immigrant clinics • Comments on DOT and Coast Guard proposed regulations • Position paper on Meaningful Use for EHRs • Dicussions with Society Occupational Medicine regarding International cooperation

ACOEM’s AGENDA FOR CHANGE Healthy Workforce Now 1. Establish a national culture of health in the workplace. 2. Ensure that every worker in the United States has access to occupational health care. 3. Protect public health and public safety by promoting workplace initiatives that help strengthen and improve the national public health and public safety infrastructure.

• 4. Improve the quality, cost and consistency of the nation’s workers’ compensation systems. • 5. Reduce health disparities in the workplace. • 6. Create stronger protections for workers through enhanced rulemaking and recordkeeping policies. • 7. Promote federal funding for training programs in OEM residency programs.

• 8. Include workplace health initiatives as a fundamental component of federal health policy. • 9. Raise awareness and response to environmental health risks in the workplace, homes and communities. • 10. Strengthen the practice environment for OEM physicians to ensure they are able to provide the full extent of their expertise to benefit the health of workers, their dependents, and retirees.

ACOEM Task Force Highlights • ACOEM Task Force on OEM Training Funding • Biosafety Lab Occupational Health Support • ACOEM as High Tech/High Touch Support Organization • 2016 Centennial: 100 years of ACOEM influence and impact

ACOEM Strategic Plan • Vision: “Pre-eminent organization of physicians who champion the health and safety of workers, workplaces and environments. ” • Mission: “ACOEM provides leadership to promote optimal health and safety of workers, workplaces, and environments by: • • • Educating health professionals and the public Stimulating research Enhancing the quality of practice Guiding workplace public policy Advancing the field of occupational and environmental medicine

ACOEM Objectives • Communicate the value of the OEM specialty – Educate our members, other professions and the payer community regarding the value of the specialty; define our markets, craft the appropriate message for each individual market and move the communication/education to the appropriate venue.

ACOEM Objectives • Promote excellence in healthcare – Foster and provide opportunities to gain and maintain knowledge and expertise in OEM

ACOEM Objectives • Enhance the practice of OEM – Provide programs to meet the operational and business/financial needs of those engaged in primarily clinical OEM (e. g. Occ Health Clinics, Urgent care Centers, On-site Clinics, etc. )

ACOEM Objectives • Enhance the value in ACOEM Membership – Increase leadership listening to our members and their customers, providing appropriate feedback to our members and addressing the needs and interests of our membership

ACOEM Objectives • Enhance organizational effectiveness – Define and separate strategic and tactical roles with a clear understanding of accountability

ACOEM Objectives • Stimulate research – Focus on cutting-edge clinical, financial and functional outcomes and environmental issues

Where are we headed? Address the pipeline Address OM training and funding - ERCs +++ Keep our members up to date Take good care of our members/potential members • ACOEM a high touch and high tech organization • Let the world know - We are Preventionists • Meet the needs and demands in the market • •

Where are we headed? • Continue to strive to point to truth in good evidence based science • Have an army long term to address the unpredictably unfolding, building and revision of HC reform • Get much better at influencing and persuading in the public policy arena • Continue to help build a model that pays for prevention and good health outcomes in addition to illness care

Where are we headed? • Build much stronger partnerships with NIOSH, CDC, OSHA, DOT and many others • Stay ahead of the technology curve and leverage it: High tech and yet high touch • Be even more engaged as members of ACOEM to make this happen • Build our future over the next 5 – 10 years as have been doing throughout our history, reinventing ourselves from industrial medicine to population health leaders

Where are we headed? • This will require each of us working together, in the most coordinated and effective ways we can offer • Pick our battles carefully and say no to wasteful and internecine skirmishes • Keep to the high ground, the greater good • So while we strive to improve the enjoyment of what we practice, to remember what we do is for those who work, and to further help to make work something which fosters health , safety and the environment.

Opportunities More jobs than ever in occupational medicine Health care reform – pay for prevention Ahead of the curve on guidelines Untapped exposure to medical students and residents • New work needs our help – nano, work overload, biosafety labs, DOT, disparities • Recall what we have built – MRO, DOT, H & P, Guidelines – keep building • •

Our Job • • • Focus on the future, our mission Deliver what we do outstandingly well Be passionate in what we do Engage talent of our members to build Manage our resources

How ACOEM Can Help • We all must work together on this agenda for the future of our specialty • ACOEM plays a key role as a hub in this effort • Beyond our work as your voice in Washington D. C. and as an advocate across the country, we are committed to providing you with the resources that will strengthen your day-to-day practice and thus enhance our shared future.

How ACOEM Can Help My. ACOEM – new, robust website ACOEM Career Center CME, Webinars, other educational resources Facilitating involvement: Council activities; Component networking • Practice tools: ACOEM Guidelines, H&P toolkit, etc. • Enhancements to doctor finder • •

ACOEM IDEA MARKETPLACE

•


See you all in Orlando • April 28 - May 1, 2013 • Rosen Shingle Creek • AOHC 2013

AOHC 2014 • April 27 - April 30, 2014 • Marriott Rivercenter • San Antonio, TX

Questions? • ACOEM wants to hear from its member and components. • ACOEM wants to learn from its members and components.

See you all in Orlando • April 28 - May 1, 2013 • Rosen Shingle Creek • AOHC 2013
fb708ce27f4df408e0bd2eacf279191d.ppt