5ea404a85fefd622be9acd8a47fe3f65.ppt
- Количество слайдов: 31


 Dr Samar Sarsam")
Abnormal labor and abnormal uterine contractions (dystocia) Dr Samar Sarsam

• • DEFINITION Dystocia is defined as difficult labor or childbirth. It may be associated with abnormalities involving: Abnormalities of the Passage Abnormalities of the Passenger Abnormalities of the Powers or a combination of these factors

• INCIDENCE • Over the last quarter of a century, the cesarean section rate in the United States has risen to approximately 25% of deliveries done each year. Dystocia is currently the most common indication for primary cesarean section, and is about three times more common than either non reassuring fetal status or malpresentation. •

•
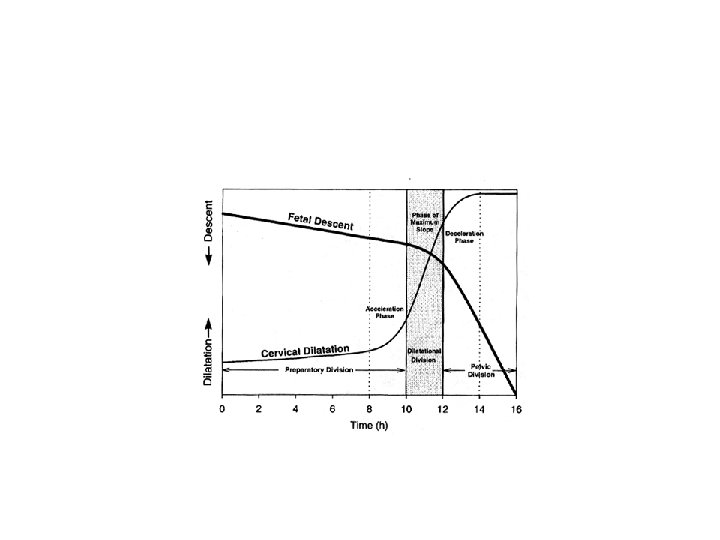
 Friedman labor curve in nulliparous 2 nd dec stage 1 st")
Cervical dilatation (cm) Friedman labor curve in nulliparous 2 nd dec stage 1 st stage max slope acceleration Active phase Latent phase Time (hours)

• ABNORMAL PATTERNS OF LABOR • The progress of labor is evaluated primarily through estimates of cervical dilatation and descent of the fetal presenting part. Normal labor patterns in primigravidas and multiparas have been described in detail by Friedman and others.
 prolonged latent phase,")
• Friedman also described four abnormal patterns of labor: (1) prolonged latent phase, (2) protraction disorders (protracted activephase dilatation and protracted descent), (3) arrest disorders (prolonged deceleration phase, secondary arrest of dilatation, arrest of descent, and failure of descent), and (4) precipitate labor disorders.

• 1. Prolonged Latent Phase • The latent phase of labor begins with the onset of regular uterine contractions and extends to the beginning of the active phase of cervical dilatation. The duration of the latent phase averages 6. 4 hours in nulliparas and 4. 8 hours in multiparas. • Causes of prolonged latent phase include: • excessive sedation or sedation given before the end of the latent phase. • labor beginning with an unfavorable cervix. • uterine dysfunction characterized by weak, irregular, uncoordinated, and ineffective uterine contractions. • fetopelvic disproportion.

Treatment options: therapeutic rest with sedation and hydration. active management of labor. 85% of patients spontaneously enter the active phase of labor. • Ten percent of patients will have been in false labor, and may be allowed to return home to await the onset of true labor if fetal status is reassuring. • In the remaining 5% of patients, uterine contractions remain ineffective in producing dilatation; in the absence of any contraindication, active stimulation of labor with oxytocin infusion may be effective in terminating the latent phase of labor. • • •

• 2. Protraction Disorders • Protracted cervical dilatation in the active phase of labor • Protracted descent of the fetus constitute the protraction disorders. • Protracted active-phase dilatation is characterized by an abnormally slow rate of dilatation in the active phase, ie, less than 1. 2 cm/h in nulliparas or less than 1. 5 cm/h in multiparas. • Protracted descent of the fetus is characterized by a rate of descent under 1 cm/h in nulliparas or under 2 cm/h in multiparas. • The second stage of labor, which normally averages 20 minutes for parous women and 50 minutes in nulliparous women, is protracted when it exceeds 2 hours in nulliparas or 1 hour in multiparas, or 3 and 2 hours respectively in the presence of conduction anesthesia.

• The underlying pathogenesis of protracted labor is probably multifactorial. • Fetopelvic disproportion. • minor malpositions such as occiput posterior. • improperly administered conduction anesthesia. • excessive sedation. • pelvic tumors obstructing the birth canal.

• Treatment of protraction disorders • Cesarean section is indicated in the presence of confirmed fetopelvic disproportion. • In the absence of fetopelvic disproportion, conservative management, consisting of support and close observation, and therapy with oxytocin augmentation both carry a good prognosis for vaginal delivery. •

• 3. Arrest Disorders • The four patterns of arrest in labor: • (1) prolonged deceleration, with deceleration phase lasting more than 3 hours in nulliparas or more than 1 hour in multiparas. • (2) secondary arrest of dilatation, with no progressive cervical dilatation in the active phase of labor for 2 hours or more. • (3) arrest of descent, with descent failing to progress for 1 hour or more. • (4) failure of descent, with descent failing to occur during the deceleration phase of dilatation and during the second stage.

• Causes: • About 50% of patients with arrest disorders demonstrate fetopelvic disproportion. • various fetal malpositions (eg, occiput posterior, occiput transverse, face, or brow). • inappropriately administered anesthesia, or excessive sedation. • If fetopelvic disproportion is established, cesarean section is done. • If fetopelvic disproportion is not present and uterine activity is less than optimal, oxytocin stimulation is generally effective in producing further progress.

• 4. Precipitate Labor Disorders • Precipitate dilatation occurs if cervical dilation occurs at a rate of 5 or more centimeters per hour in a primipara or at 10 cm or more per hour in a multipara. Precipitate descent occurs with descent of the fetal presenting part of 5 cm or more per hour in primparas and 10 cm or more per hour in multiparas.

• • • Causes: 1 -extremely strong uterine contractions 2 -low birth canal resistance. abnormal contractions may be associated with administration of oxytocin and abruptio placentae. If oxytocin administration is the cause of abnormal contractions, it may simply be stopped. The problem typically resolves in less than 5 minutes. If excessive uterine activity is associated with fetal heart rate abnormalities, and this pattern persists despite discontinuation of oxytocin, a b-mimetic such as terbutaline or ritodrine can be given and magnesium sulfate also Lacerations of the birth canal are common. maternal amniotic fluid embolism. predisposing to postpartum hemorrhage. Perinatal mortality is increased secondary to hypoxia, possible intracranial hemorrhage, and risks associated with unattended delivery.
. soft tissue")
PATHOGENESIS & TREATMENT --Abnormalities of the Passage Causes: bony abnormalities (pelvic dystocia). soft tissue obstruction of the birth canal. abnormal placental location. Pelvic dystocia, is the most common cause of passage abnormalities. • The etiology and diagnosis of pelvic abnormalities begins with the shape, classification, and clinical assessment of the adult female pelvis. . • Ultrasound, magnetic resonance imaging (MRI), and xrays have been used to investigate pelvic size and shape for evidence of pelvic contraction obstructing the normal progress of labor. • •

• X-ray pelvimetry has now fallen into limited use. • Clinical pelvimetry has been largely used in the routine evaluation of most obstetric patients. • The diagnosis of fetopelvic disproportion has generally become a diagnosis of exclusion, after fetal factors and uterine dysfunction have been ruled out. • However, x-ray pelvimetry retains a role in the evaluation of a pelvis for the feasibility of vaginal breech delivery and in the assessment of gross bony distortion such as previous pelvic fracture or rachitic deformity. • Contractions of the pelvis are generally classified as: • contractions of the inlet, midpelvis, or outlet, or as a combination of these elements.

• Inlet contraction is suspected if the anteroposterior diameter of the pelvis is less than 10 cm, the transverse diameter is under 12 cm, or both. • floating vertex presentation with no descent during labor, • abnormal presentation, • prolapsed cord or extremity. • considerable molding of the fetal head, • caput succedaneum formation, • and prolonged rupture of the membranes. • If allowed to continue, abnormal thinning of the lower uterine segment may occur, with development of a Bandl's retraction ring, or even frank uterine rupture. • Cesarean section is the treatment of choice in true inlet contraction.

• Midpelvis contraction it is more frequent than inlet dystocia because the midpelvis is smaller than the inlet and positional abnormality is more common at this level. • Presentation: • Arrest of descent • Poor application of the head to the cervix • Abnormal rate of cervical dilatation • Contraction of the outlet is extremely unusual unless found in association with a Midpelvis contraction. • Criteria for assessing pelvic outlet adequacy include intertuberous diameter greater than 8 cm and a sum of the intertuberous diameter and the anteroposterior diameter greater than 15 cm.

• Midpelvic outlet obstruction is detected clinically on the basis of convergent side walls, prominent ischial spines, or a narrow pelvic arch. • It may present as a prolonged second stage, • persistent occiput posterior position, • deep transverse arrest. • Molding of the fetal head and caput succedaneum formation are common.

• Uterine rupture may occur in prolonged labor complicated by midpelvic outlet obstruction, and vesicovaginal or rectovaginal fistula formation may result with pressure necrosis of the surrounding tissues of the birth canal by the fetal head. • Cesarean section is therefore the delivery method of choice in this complication. • Other anatomic abnormalities of the reproductive tract may cause dystocia is soft tissue dystocia may be caused by uterine or vaginal congenital anomalies, scarring of the birth canal, pelvic masses, or low implantation of the placenta.

• --Abnormalites of the Passenger • **A. malposition and malpresentation: • Fetal malpresentations are abnormalities of fetal position, presentation, attitude, or lie. They collectively constitute the most common cause of fetal dystocia, occurring in approximately 5% of all labors. • 1. Vertex malpositions— • a. Occiput posterior— • b. Occiput transverse— • 2. Brow presentation—Brow presentations usually are transient fetal presentations with deflexion of the fetal head.

• 3. Face presentation—In face presentation, the fetal head is fully deflexed from the longitudinal axis. • 4. Abnormal fetal lie—In transverse or oblique lie, the long axis of the fetus is perpendicular to or at an angle to the maternal longitudinal axis.

• 5. Breech presentation • **B. fetal macrosomia • **C. fetal malformation • The most common malformation is hydrocephalus, enlargement of the fetal abdomen caused by distended bladder, ascites, or abdominal neoplasms; or other fetal masses, including meningomyelocele or cystosarcoma.
")
• Abnormalities of the Powers • Normal uterine activity during labor: • (1) the relative intensity of contractions is greater in the fundus than in the midportion or lower uterine segment (this is termed fundal dominance); (2) the average value of the intensity of contractions is more than 24 mm Hg. (3) contractions are well synchronized in different parts of the uterus; (4) the basal resting pressure of the uterus is between 12 and 15 mm Hg; (5) the frequency of contractions progresses from one every 3– 5 minutes to one every 2– 3 minutes during the active phase; (6) the duration of effective contraction in active labor approaches 60 seconds; and (7) the rhythm and force of contractions are regular.

• Quantification of uterine activity during labor by: • -external tocodynamometry • -intrauterine pressure catheter measurement. • Uterine dysfunction generally comprises 3 categories: • hypotonic dysfunction, • hypertonic dysfunction, • uncoordinated dysfunction.

• Hypotonic dysfunction is uterine activity characterized by contraction of the uterus with insufficient force (> 24 mm Hg), irregular or infrequent rhythm, or both. Seen most often in primigravidas in the active phase of labor, it may be caused by excessive sedation, early administration of conduction anesthesia, twins, polyhydramnios, or overdistention of the uterus. • Hypotonic dysfunction responds well to oxytocin; however, care must be taken to first rule out cephalopelvic disproportion and malpresentation. Active management of labor has been shown to decrease perinatal morbidity and cesarean section rates.

• hypertonic uterine contractions and uncoordinated contraction often occur together and are characterized by elevated resting tone of the uterus, dyssynchronous contractions with elevated tone in the lower uterine segment, and frequent intense uterine contractions. It is generally associated with abruptio placentae, overuse of oxytocin, cephalopelvic disproportion, fetal malpresentation, and the latent phase of labor. • Treatment: • tocolysis, decrease in oxytocin infusion • cesarean section as indicated for concomitant malpresentation, cephalopelvic disproportion, or fetal distress.

• When these patterns occur in the latent phase of labor: • sedation may be effective in converting hypertonic contractions to normal labor patterns. • Inadequate pushing in the second stage of labor is common and may be caused by conduction anesthesia, oversedation, exhaustion, or neurologic dysfunction such as paraplegia or hemiplegia of various causes, or by psychiatric disorders. • Mild sedation may improve expulsive efforts. • outlet forceps or vacuum delivery may be of help.
5ea404a85fefd622be9acd8a47fe3f65.ppt