ad9c9051200433d026efa029f9f00267.ppt
- Количество слайдов: 88



abcd The 2002 Healthcare Conference 29 September-1 October 2002 Scarman House, The University of Warwick, Coventry

Session B 1 : Critical Illness n Trends in Critical Illness n Heart Attack & Stroke n Working Party / Research Sub-group Report n Scott Reid & Joanne Wells

Critical Illness Trends Working Party Our Aims : n To examine underlying trends in the factors influencing UK Insured Critical Illness claim rates, and from these, to assess : n The historic trend in incidence and death rates for the major CI’s n Any pointers for future trends in Standalone CI, Mortality and hence Accelerated CI. n Formed in March 2001

Sub-Group Members n Actuaries Scott Reid Joanne Wells n Medical Expert Dr Richard Croxson - Consultant Cardiologist

Contents Slide n n n Background and set the scene Variations by deprivation category Variations by ICD code Impact of smoking Future influences on rates Project population incidence rates

Contents Slide n n n Background and set the scene Variations by deprivation category Variations by ICD code Impact of smoking Future influences on rates Project population incidence rates

Background and set the scene n Re-cap of previous work n Data sources used n Scottish n English n Next step forward

Background and set the scene n Re-cap of previous work n Data sources used n Scottish n English n Next step forward

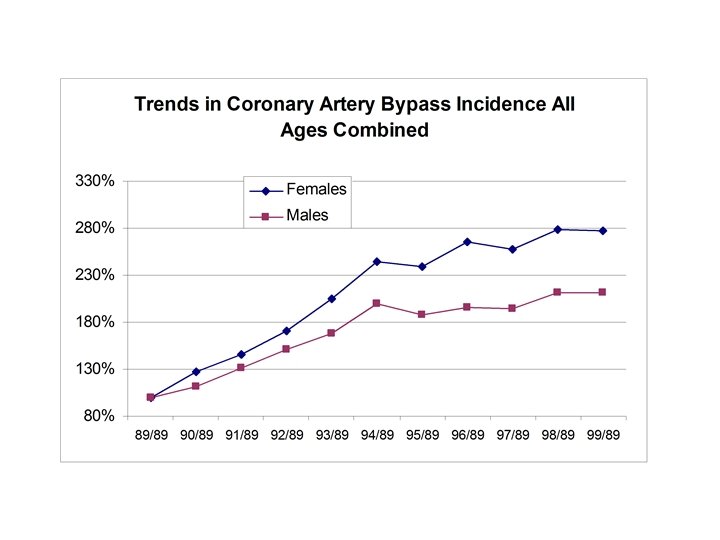
Re-cap of previous work n Population trends – Scotland England n n Heart attack Stroke CABG Angioplasty n Broad brush analysis of smoker prevalence

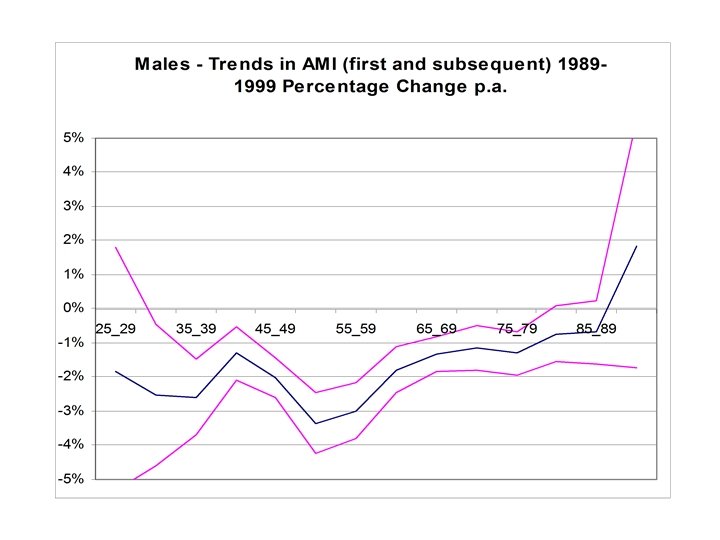
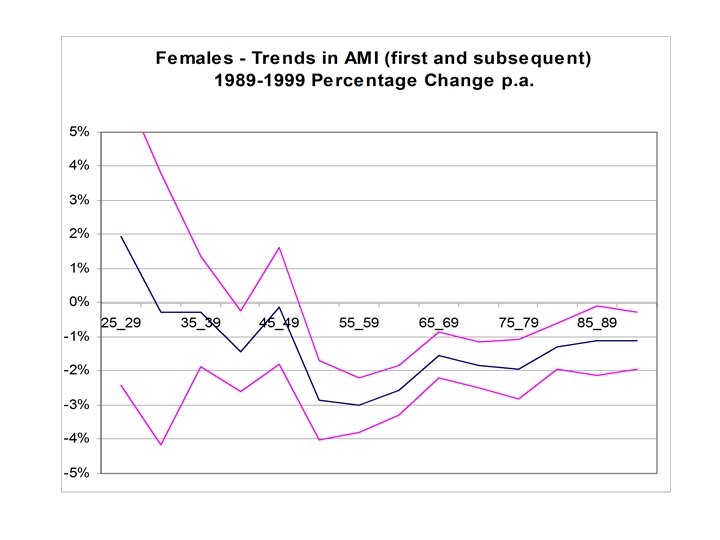
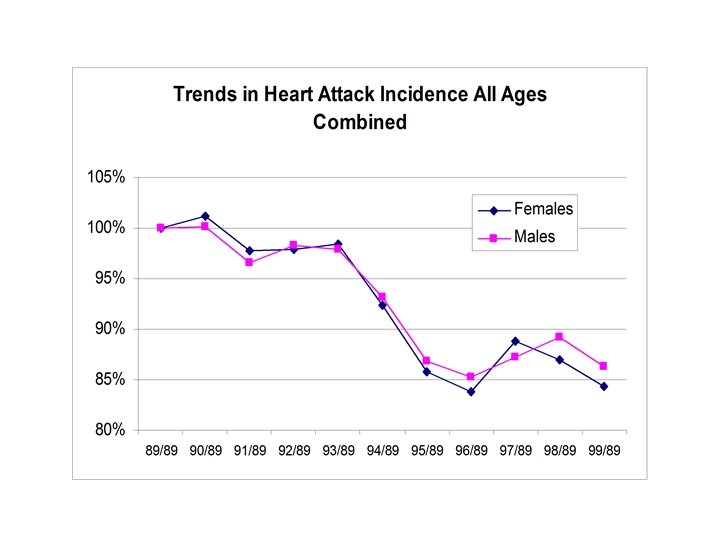
Population trends – Scotland England n Heart attack n Significant mortality and incidence improvements n Scottish rates at a significantly higher level n Stroke n English data unclear n Scottish data n Flat trend during 1980’s n Deterioration during early 1990’s

Broad brush analysis of smoker prevalence n Smoking is a key risk factor n Reduction in smoking prevalence n Scottish and English smoker prevalence patterns n Scottish trends

Background and set the scene n Re-cap of previous work n Data sources used n Scottish n English n Next step forward

Data sources used n Scottish population – ISD data n Good quality n Patient based n English population - HES data n Data quality is questionable n Episode based

Background and set the scene n Next step n n n Insured trends Understanding the main drivers to cause trends Smoker differentiated rates Future influences Overall trend pattern

Contents Slide n n n Background and set the scene Variations by deprivation category Variations by ICD code Impact of smoking Future influences on rates Project population incidence rates

Variations by deprivation class n n Why split by deprivation class? Data sources used Explanation of deprivation scores and categories Overall trends by gender n Heart attack n Stroke n Conclusion

Variations by deprivation class n n Why split by deprivation class? Data sources used Explanation of deprivation scores and categories Overall trends by gender n Heart attack n Stroke n Conclusion

Why split by deprivation class? n To understand trend at insured level n Regional variations and Target market variations n Understand the main drivers of health inequalities n Black report 1980: “. . the main influence on the inequalities in health which were observed lay in the material circumstances in which people live” n Deprivation and Health in Scotland, 1991 (Carstairs & Morris) n Classification by postcode; overcomes the weakness of Occupational classification.

Variations by deprivation class n n Why split by deprivation class? Data sources used Explanation of deprivation scores and categories Overall trends by gender n Heart attack n Stroke n Conclusion

Data sources used n Incidence data n SMR 1/01, Information Statistics Division NHS Scotland n General Registers Office for Scotland n Mortality data n General Registers Office for Scotland n Population data n 1981 Population Census n 1991 Population Census n Split by n n n CI condition ICD code Gender 5 year age bands deprivation category

Variations by deprivation class n n Why split by deprivation class? Data sources used Explanation of deprivation scores and categories Overall trends by gender n Heart attack n Stroke n Conclusion

Explanation of deprivation scores and categories n Carstairs & Morris 1991 deprivation categories n Four indicators – to derive a composite score n Overcrowding n Male unemployment n Low social class n No car n Deprivation score divided into 7 separate categories n 1 – the most affluent group n …… n 7 – the most deprived group

Explanation of deprivation scores and categories

Explanation of deprivation scores and categories

Variations by deprivation class n n Why split by deprivation class? Data sources used Explanation of deprivation scores and categories Overall trends by gender n Heart attack n Stroke n Conclusion

Trends in incidence of first heart attack for males in Scotland, as a % of 1981 Value, 1981 to 2000

Trends in incidence of first heart attack for males in Scotland, as a % of 1981 Value, 1981 to 2000

Trends in incidence of first heart attack for males in Scotland, as a % of 1981 Value, 1981 to 2000

Trends in incidence of first heart attack for males in Scotland, per 100000 of population, 1981 to 2000

Trends in incidence rate of first heart attack for males aged 40 to 64 in Scotland, per 100000 of Population, 1981 to 2000

Trends in incidence rate of first heart attack for males aged 40 to 64 in Scotland, as a % of 1986 Value, 1981 to 2000

Trends in incidence rate of first heart attack for females aged 40 to 64 in Scotland, per 100000 of Population, 1981 to 2000

Trends in incidence rate of first heart attack for females aged 40 to 64 in Scotland, as a % of 1986 Value, 1981 to 2000

Summary of heart attack trends by deprivation class

Summary of heart attack trends by deprivation class, Males aged 40 to 64, 1986 to 2000

Summary of heart attack trends by deprivation class, Males aged 40 to 64, 1986 to 2000

Brief interpretation of heart attack trends Male Mortality Female Positive correlation between affluent and deprived groups Incidence Less clear. Weak negative correlation where deprived group has higher improvement Postive correlation between affluent and deprived groups except for categories 6 and 7

Variations by deprivation class n n Why split by deprivation class? Data sources used Explanation of deprivation scores and categories Overall trends by gender n Heart attack n Stroke n Conclusion

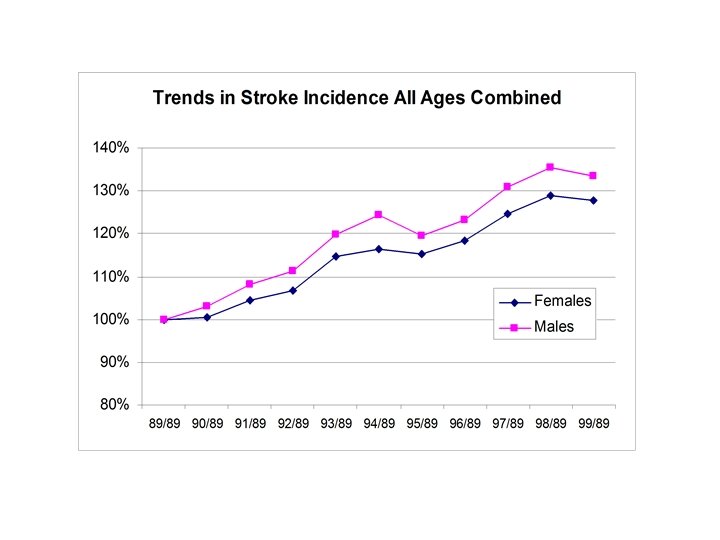
Trends in incidence rate of first stroke for males aged 40 to 64 in Scotland, as a % of 1981 value, 1981 to 2000

Trends in incidence rate of first stroke for males aged 40 to 64 in Scotland, as a % of 1981 value, 1981 to 2000

Trends in incidence rate of first stroke for males aged 40 to 64 in Scotland, as a % of 1981 value, 1981 to 2000

Trends in incidence rate of first stroke for males aged 40 to 64 in Scotland, per 100000 of Population, 1981 to 2000

Trends in incidence rate of first stroke for males aged 40 to 64 in Scotland, per 100000 of Population, 1986 to 2000

Trends in incidence rate of first stroke for females aged 40 to 64 in Scotland, per 100000 of Population, 1986 to 2000

Trends in mortality rate by stroke for males aged 40 to 64 in Scotland, per 100000 of Population, 1986 to 2000

Trends in mortality rate by stroke for females aged 40 to 64 in Scotland, per 100000 of Population, 1986 to 2000

Summary of stroke trends by deprivation class

Summary of stroke trends by deprivation class, Males aged 40 to 64, 1986 to 2000

Summary of stroke trends by deprivation class, Females aged 40 to 64, 1986 to 2000

Brief interpretation of stroke trends Male Female Mortality Positive correlation Weak negative between affluent and correlation between deprived groups affluent and deprived groups Incidence Weak positive Weak postive correlation between affluent and deprived groups

Contents Slide n n n Background and set the scene Variations by deprivation category Variations by ICD code Impact of smoking Future influences on rates Project population incidence rates

Variation by ICD code n Why? n Understanding of overall rate n Explain which components have influenced overall trend n Heart attack n ICD 9 code 410 n Unstable angina ICD 9 code 413 n Stroke n ICD 9 codes 430 to 437 excluding 435

Variation by ICD code n Why? n Understanding of overall rate n Explain which components have influenced overall trend n Heart attack n ICD 9 code 410 n Unstable angina ICD 9 code 413 n Stroke n ICD 9 codes 430 to 437 excluding 435

Trend in first incidence rate for males aged 40 to 64 by ICD code 410 and 413, per 100000 of Population, 1981 to 2000

Trend in first incidence rate for females aged 40 to 64 by ICD code 410 and 413, per 100000 of Population, 1981 to 2000

Variation by ICD code n Why? n Understanding of overall rate n Explain which components have influenced overall trend n Heart attack n ICD 9 code 410 n Unstable angina ICD 9 code 413 n Stroke n ICD 9 codes 430 to 437 excluding 435

Trend in first incidence rate for males aged 40 to 64 by ICD codes 430 to 437 excluding 435, per 100000 of Population, 1981 to 2000

Trend in first incidence rate for males aged 40 to 64 by ICD codes 430 to 437 excluding 435, 1981 to 2000

Trend in first incidence rate for females aged 40 to 64 by ICD code 430 to 437 excluding 435, per 100000 of Population, 1981 to 2000

Trend in first incidence rate for females aged 40 to 64 by ICD code 430 to 437 excluding 435, per 100000 of Population, 1981 to 2000

Summary of variation by ICD code n Heart attack: n ICD 410 is improving over time (Male 3. 6% p. a. , Female 3. 3%) n ICD 413 is deteriorating (Male 5. 2% p. a. , Female 6. 2% p. a. ) n Troponins? n Stroke n Large component ICD 436 is improving over time (Male 5. 2% p. a. , Female 6. 2%) n Remaining components ICD 430, 431, 432, 433, 434, 437 overall are deteriorating over time (Male 5. 7% p. a. , Female 4. 3% p. a. ) n Overall deterioration (Male 1. 9%, Female 1. 5%) n Overall flat trend over 1980’s, deterioration over 1990’s n Future?

Contents Slide n n n Background and set the scene Variations by deprivation category Variations by ICD code Impact of smoking Future influences on rates Project population incidence rates

Contents Slide n Introduction n Variations by deprivation category n Variations by ICD code n Impact of smoking n Future influences on rates n Projecting population incidence rates
 = ix(ns)* p(ns) +")
Impact of Smoking - “Ideal” Smoking Model n ix (pop) = ix(ns)* p(ns) + ix (s) * p(s) +ix(ex) * p(ex) n ix (pop) = ix(ns)* p(ns) + ix (s) * p(s) + t ix(ex t) * p(ex t) n …. .

Impact of Smoking - Data Available n Epidemiological evidence on smoking n Case control studies, prospective cohort studies etc n Wide range of results n results become even more volatile if looking for age specific or duration smoked/quit specific results n often look at impact on mortality not incidence n cause investigated is often not an exact match e. g. coronary heart disease and not acute myocardial infarction n usually smoking status is only investigated at the start of the study period n Simplify and/or use proxies

Impact of Smoking - Data Available n Epidemiological evidence on smoking n Case control studies, prospective cohort studies etc n Wide range of results n results become even more volatile if looking for age specific or duration smoked/quit specific results n often look at impact on mortality not incidence n cause investigated is often not an exact match e. g. coronary heart disease and not acute myocardial infarction n usually smoking status is only investigated at the start of the study period n Simplify and/or use proxies
 = ix(ns)*")
Impact of Smoking -Smoking Model n Age specific model n ix (pop) = ix(ns)* propx (ns) + ix (ns) * RRx *propx (s) n assumes that people move immediately from being a smoker to a never smoker n Ex-smoker model n ix(pop) = ix(ns) *propx(ns) + ix(ns) * RR 1 *propx (ex 1) +… n ……. + ix(ns) *RR(sm) propx(s) n assumes that the relative risks for smokers and ex-smokers are independent of age

Impact of Smoking - Males

Impact of Smoking - Females

Contents Slide n Introduction n Variations by deprivation category n Variations by ICD code n Impact of smoking n Future influences on rates n Projecting population incidence rates

Future Influences on Rates n Impact of changing risk factors on incidence n Focus on changes in diagnostic techniques and potential shocks in incidence n Discussion of impact of troponin on heart attack incidence n Interpreting trends in stroke incidence and the potential impact of brain imaging techniques

Troponin and Acute Coronary Syndrome n Number of medical papers available n Generally look at the change in the number of diagnoses in the spectrum of ACS

Spectrum of Acute Coronary Syndromes K Fox. , Heart; 2000; 84; 93 -100

Troponin and Acute Coronary Syndrome n Number of medical papers available n Generally look at the change in the number of diagnoses in the spectrum of ACS n As might be expected sample sizes quite small n Definitions do not exactly match those used by the insurance industry n Average is considerably higher than that of people who claim for critical illness

Troponin and Acute Coronary Syndrome

Troponin and Critical Illness n Medical studies give a range of results n Results need careful interpretation before trying to apply them to critical illness n More AMI being diagnosed but some an acceleration e. g. n subsequent heart attack n coronary artery bypass surgery

Troponin and Critical Illness n Percentage of hospitals where troponin is available n Scotland - 70% (Pell BMJ Vol 324) n England - 60% last year thought to be 70% to 80% this year n No clear consensus amongst cardiologists in the UK on the definition n New definition not disseminated until September 2000 so no effect on the data currently published

Stroke - Identifying Trends “Stroke mortality is falling in many countries, but it is unclear whether this is due to a fall in stroke incidence, lower case fatality, or some artifact of the collection and analysis of routine mortality data. ” Stroke, A Practical Guide and Management. Warlow et al

Stroke - Identifying Trends “In the few places where it has been measured reasonably reliably, stroke incidence seems to have declined, stayed the same, or increased. However it has been very difficult to use consistent methods and obtain large enough data sizes for precise estimates. In truth it is not very clear what incidence rates are doing. ” Stroke, A Practical Guide and Management. Warlow et al

Stroke - HES Data g Patients admitted to hospital generally have more severe strokes n The proportion of all strokes admitted is unknown and can change over time n Cannot identify first ever strokes n Double counting as patients move from one hospital service to another n Question mark over change in incidence coinciding with coding change

Stroke - Diagnosis n ABI definition of stroke is different to that used by clinicians and to that used by the WHO n Consequences of, for example, increased MRI scanning could have a different impact under different definitions n Will policyholders understand the differences? n Milder strokes more often identified? n Patient expectations are rising n Diagnostically more competent n Helped by more sensitive brain imaging

Contents Slide n Introduction n Variations by deprivation category n Variations by ICD code n Impact of smoking n Future influences on rates n Projecting population incidence rates

Population - Projection of Incidence Rates
ad9c9051200433d026efa029f9f00267.ppt