55067369c3cf2bf0a91d39063fca5630.ppt
- Количество слайдов: 116




A formal process of obtaining a complete and accurate list of each patient’s current medications At Admission, Discharge and at all other Transitions in Care

• Chart reviews have revealed over half of all hospital medication errors occur at the interfaces of care • Medication errors are one of the leading causes of injury to hospital patients

• 2004 Canadian Adverse Events Study – Drug and fluid related events were the second most common type of procedure or event to which adverse events were related • 2004 Study in Canadian Hospital – 23% incidence of adverse events in patients discharged from an internal medicine service • 72% were medication related

• 2005 Canadian Study – 151 General Medicine patients • Prescribed or receiving at least four medications • Not from an extended care facility – 53. 6% - Patients 1 Unintentional Discrepancy • 38. 6% - Potential to cause moderate or severe discomfort or clinical deterioration • 46. 4% - Omission of regularly used medication

• Canadian Council on Health Services Accreditation – Patient Safety Goals & Required Organization Practices for 2005 • “Reconcile the patients’ medications upon admission, and with the involvement of the patient” • “Reconcile medications with the patient at referral or transfer and communicate the patients’ medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization”

• “Desirable continuity of care delivered to a patient in the health care system across the spectrum of caregivers and their environment” • “When moving between levels of care, patients’ drug information is not always transferred to all care providers in a timely fashion… consequently, the patient may not receive the most appropriate regimen for their condition of this seamless care process” Medication Reconciliation is a key component of the Seamless Care process

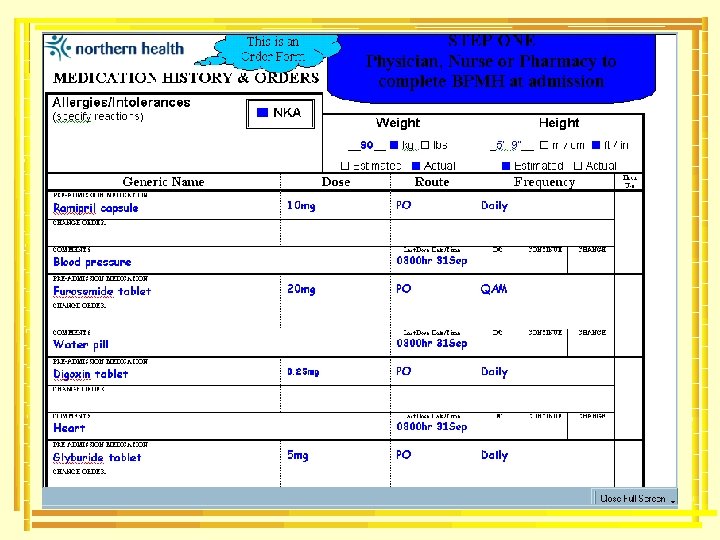
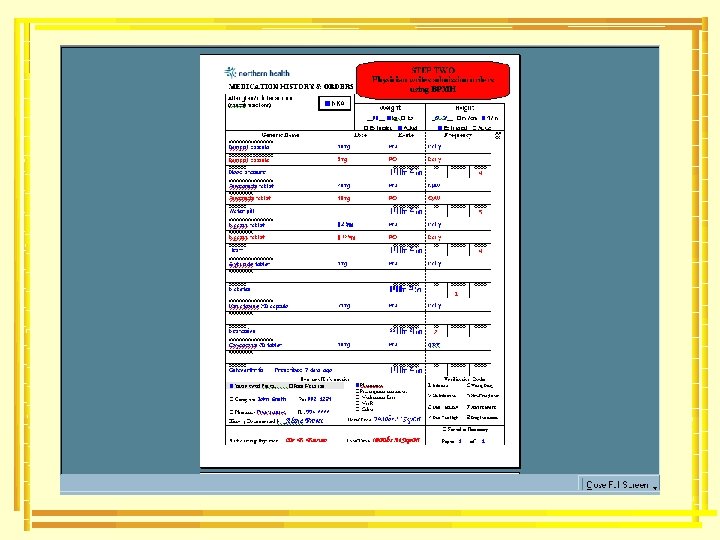
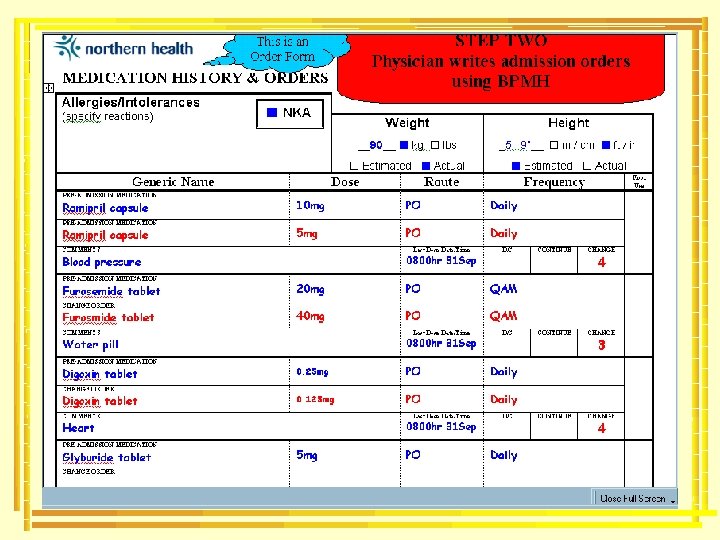
Easy as 1 -2 -3 1. Create the most complete and accurate list possible of all current medications 2. Use this list when writing medication orders 3. If using this process after admission orders have been written, reconcile and resolve any discrepancies

An accurate medication history is performed prior to physician admission order writing An accurate medication history is performed after physician admission order writing This history is used to write admission orders This history is compared to admission orders and any discrepancies are reconciled PREVENTS ERRORS CATCHES ERRORS

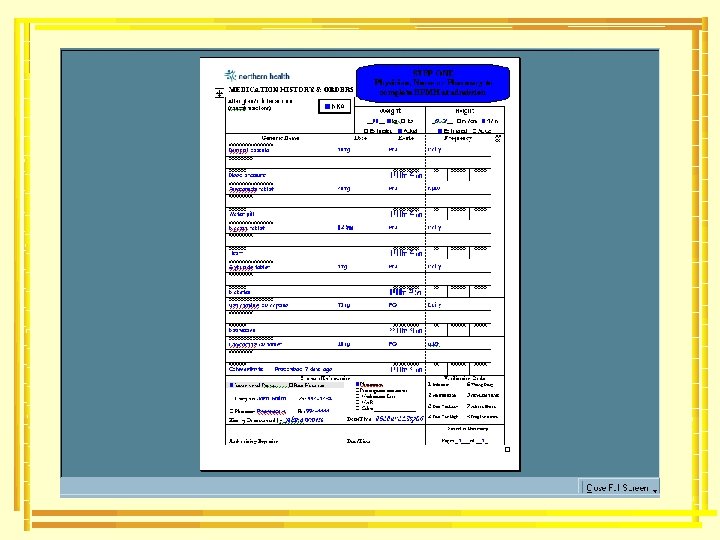
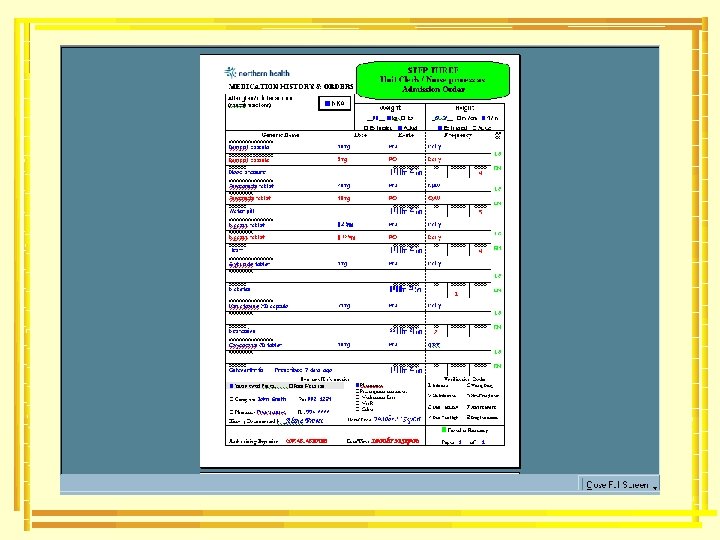
Nurse/Physician/Pharmacy performs medication history at time of admission and prior to admission orders being written Medication History & Orders Form used to document medication history Medication history documented in traditional locations in the patient’s chart Physician uses Medication History & Orders Form to indicate continuation, discontinuation or change to pre-admission medications. Any others admission orders are written on usual physician order sheet Physician uses usual physician order sheet to write admission orders Orders are processed to pharmacy using Medication History & Orders Form for any pre-admit medications and using the physician’s order sheet for new admission orders Orders are processed to pharmacy using usual physician order sheet Pharmacy dispensary receives the orders and processes as usual If a Medication History & Orders Form was completed in the admission order writing process, no further medication reconciliation is required All patient admitted without a completed Medication History & Orders Form will be assessed using the Assessment of Patient Risk (APR) Tool to determine all high risk patients requiring the completion of a Medication Reconciliation process
 Tool will be")
Patients deemed high risk using the Assessment of Patient Risk (APR) Tool will be referred to the Clinical Pharmacy team The Medication History & Orders Form will be used as a worksheet to collect and document the medication history. (Additional patient may be audited if time permits)

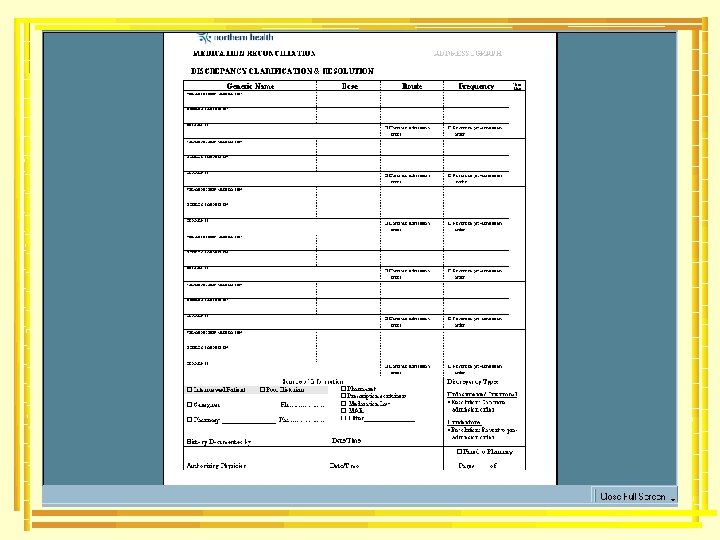
Clinical Pharmacy team will compare admission orders to medication history using the Medication History & Orders Form as a worksheet to document any discrepancies. If potential discrepancies are identified, a Discrepancy Clarification & Resolution Form will be completed and will be referred to the Clinical Pharmacist along with a copy of the Medication History Worksheet

The Clinical Pharmacist will review potential discrepancies and determine urgency to clarify. If not urgent, the Discrepancy Clarification & Resolution Form will be placed on the patient’s chart for completion by the physician upon his/her next visit. If urgent, the pharmacist will contact the physician by phone to clarify and will write verbal orders onto the Discrepancy Clarification & Resolution Form and will place in the patient’s chart to be processed as an order.

The Clinical Pharmacy team will review patient charts daily and will follow until all discrepancies are resolved. Once physician clarifies discrepancies, Clinical Pharmacy team will classify the outstanding discrepancies on the Medication History Worksheet and will file. All statistics will be compiled and reported in a monthly report.

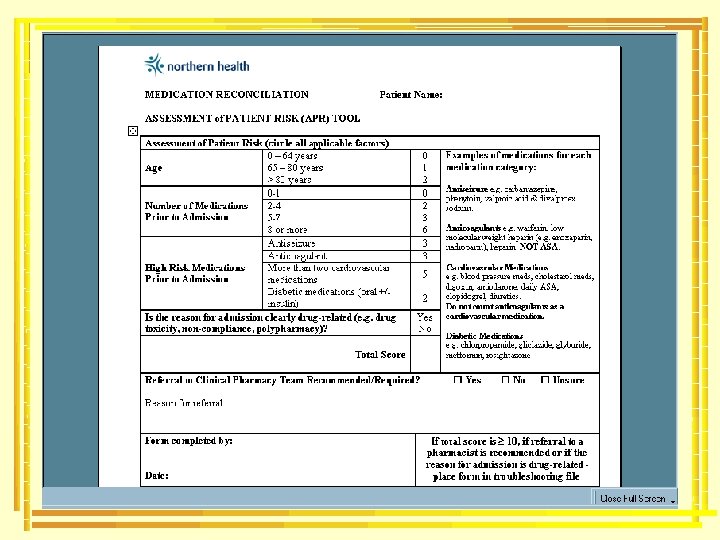
• To reconcile patients within 24 hours of admission • At a minimum, target “high-risk” patients identified using the Assessment of Patient Risk (APR) Tool Reconcile patients who have scored 10 or have been admitted as a result of a drug-related problem • If time permits, set a goal to reconcile as many patients as possible, if not ALL

 0 – 64 years 0 65")
Assessment of Patient Risk (circle all applicable factors) 0 – 64 years 0 65 – 80 years 1 > 80 years 2 Age 5 -7 8 or more ed er id k ns is co h R ig 2 -4 0 H Number of Medications Prior to Admission ot N 0 -1 2 3 6 Antiseizure Anticoagulant 3 More than two cardiovascular medications 5 Diabetic medications (oral +/- insulin) High Risk Medications Prior to Admission 3 2 Is the reason for admission clearly drug-related (e. g. drug toxicity, non-compliance, polypharmacy)? Total Score Yes No 9

• Antiseizure • carbamazepine, phenytoin, valproic acid & divalproex sodium. • Anticoagulants • warfarin, low molecular weight heparin (e. g. enoxaparin, nadroparin), heparin. • NOT ASA. • Diabetic medications • Chlorpropamide, gliclazide, glyburide, metformin, rosiglitazone • Cardiovascular Medications • blood pressure meds, cholesterol meds, digoxin, amiodarone, daily ASA, clopidogrel, diuretics. • Do not count anticoagulants as a cardiovascular medication.
 0 – 64 years 0 65")
Assessment of Patient Risk (circle all applicable factors) 0 – 64 years 0 65 – 80 years 1 > 80 years 2 Age 2 -4 5 -7 8 or more ig H ed er k sid Ris on Number of Medications Prior to Admission C 0 -1 0 2 3 6 h Antiseizure Anticoagulant 3 More than two cardiovascular medications 5 Diabetic medications (oral +/- insulin) High Risk Medications Prior to Admission 3 2 Is the reason for admission clearly drug-related (e. g. drug toxicity, non-compliance, polypharmacy)? Total Score Yes No 0
 0 – 64 years 0 65")
Assessment of Patient Risk (circle all applicable factors) 0 – 64 years 0 65 – 80 years 1 > 80 years 2 Age 2 -4 5 -7 8 or more ig H ed er k sid Ris on Number of Medications Prior to Admission C 0 -1 0 2 3 6 h Antiseizure Anticoagulant 3 More than two cardiovascular medications 5 Diabetic medications (oral +/- insulin) High Risk Medications Prior to Admission 3 2 Is the reason for admission clearly drug-related (e. g. drug toxicity, non-compliance, polypharmacy)? Total Score Yes No 10

Referral to Clinical Pharmacy Team Recommended/Required? Yes No Unsure Reason for referral: Example #1: Patient experiencing digoxin toxicity Example #2: Scored 12 Form completed by: Alana Froese Date: Today’s Date If total score is 10, if referral to a pharmacist is recommended or if the reason for admission is drug-related - place form in troubleshooting file

Case Study: Carol Harrison • Admitted to Emergency Department at 0800 hr with palpitations, tremor and flushing • Apparently patient thought her theophylline was acetaminophen extra strength and took two tablets at approximately 0400 hr • Review her Pharmanet record and determine if she is considered “high risk” and a candidate for Medication Reconciliation

Carol Harrison Admitted for drug-related problem – excess use of theophylline Alana Froese Today’s Date


Definition A medication history obtained by a healthcare professional which includes a thorough history of all regular medication use (prescription and non-prescription)

• • Patient – best source if patient competent Caregiver Pharmanet Prescription vials/Compliance packaging Medication List Pharmacy Family Physician MAR from previous institution

• Print Pharmanet record • Addressograph Forms • Determine if patient is capable of providing med history

• Pharmanet is simply a record of the DISPENSING HISTORY – Does not indicate the medications discontinued or active or if the patient is taking the medications as prescribed – Does not include HIV/AIDS medications – Does not include samples given to patients in doctor offices – Does not include physician office changes (without writing a prescription) – Does not include medications given in hospitals • Medinet is a provider of Pharmanet info
 Name Date of Birth Sex")
Demographics PHN – Personal Health Number (Care Card #) Name Date of Birth Sex

Clinical conditions Typically this area is not used Reported by Date reported

Allergies and Reactions Can not guarantee this is an accurate listing of allergies Reported by: Date reported PRACTITIONER CODES V 9 Veterinarian 91 Physician/Surgeon 95 Dentist P 1 Pharmacist 93 Podiatrist 98 Midwife
 -Drug Identification Number (DIN)")
Dispensing History -Most recent reported first -Drug by generic name(s) -Drug Identification Number (DIN) -Quantity -Sig (Instructions) -Physician -Date Filled or Reversed

• Review entire dispensing history • Multidoctoring? – scan for number of physicians dispensing • Non-compliance? – are chronic meds being filled at regular intervals • Consider how much of the history to print – Look for intermittently used medications that may still be considered active orders and ensure they are included when printed » Salbutamol MDI 2 puffs q 4 h prn » Topical creams
, searching")
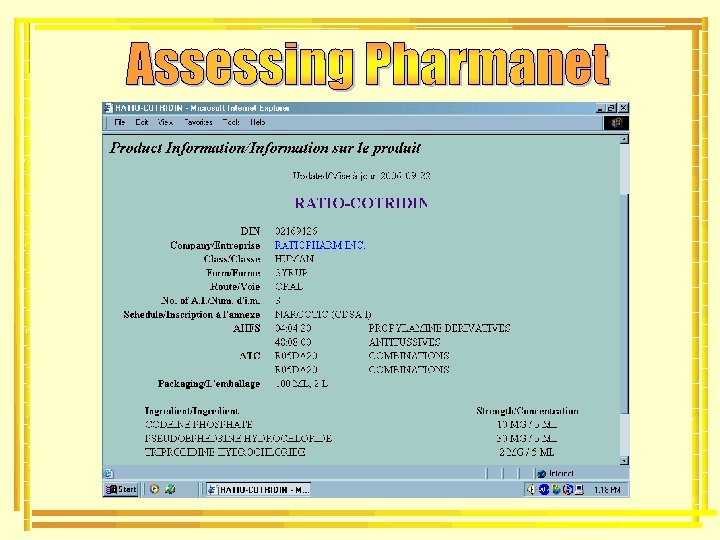
• If you can not identify a drug by its generic name(s), searching Canada’s Drug Product Database using the Drug Identification Number (DIN) will help you identify the brand name and manufacturer – http: //www. hc-sc. gc. ca/hpb/drugs-dpd/ 2169126 250 @ 8. 333/day Filled: P-EPHED HCL/CODEINE/TRIPROL RATIOPHARM 30 -10 -2/5 LIQUID TAKE 5 TO 10 ML EVERY 6 HOURS AS NEEDED 2006 Mar 29 91/03361 (LAVOY) Ratio – Cotridin
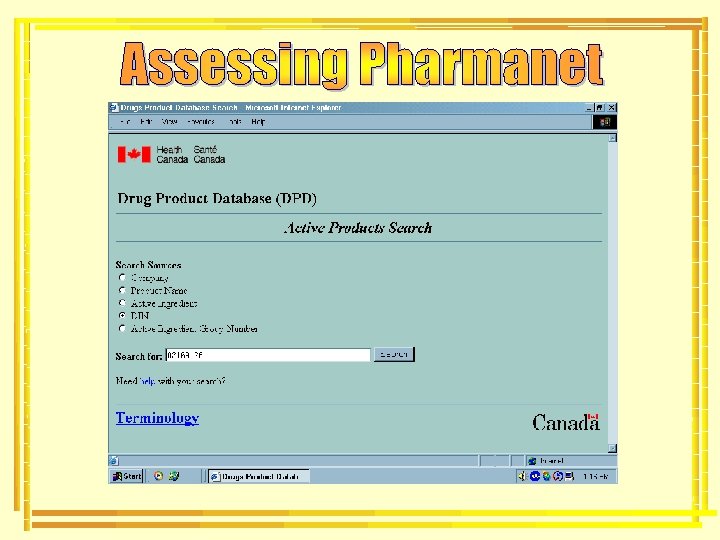

• What’s in the Drug name – List of active chemical entities • Generic name(s) – Sometimes includes secondary name • Example: Salts of Erythromycin base • Estolate, Ethylsuccinate, Lactobionate – Additional product information • Strength & Formulation – Listed between the name and strength of the product • Manufacturer 21016 60 @ 1/day Filled: QUININE SULFATE NOVOPHARM LTD 300 MG CAPSULE TAKE ONE CAPSULE AT BEDTIME AS NEEDED FOR LEG CRAMPS 2005 Dec 04 91/02295 (MACKAY)

• Watch for specialty formulation information 2014165 90 @ 1/day Filled: THEOPHYLLINE ANHYDROUS PURDUE PHARMA 400 MG TAB SR 24 H TAKE ONE TABLET ONCE DAILY 2006 Mar 04 91/02295 (MACKAY) 02202441 56 @ 2/day Filled: OXYCODONE PURDUE PHARMA 10 MG TABLET CR TAKE ONE TABLET EVERY 12 HOURS 2006 May 22 91/05568 (BROWN) 2007959 90 @ 1/day Filled: ACETYLSALICYLIC ACID PHARMASCIENCE 81 MG TABLET DR TAKE ONE TABLET ONCE DAILY 2006 Mar 04 91/02295 (MACKAY) 2237280 60 @ 1/day Filled: Sustained Release Controlled Release VENLAFAXINE WYETH CANADA 75 MG CAPSULE XR TAKE ONE CAPSULE ONCE DAILY 2006 Apr 15 91/05568 (BROWN) Delayed Release Extended Release

• Time commitment – Goal 15 min • Confirm positive identification of patient • Introduce yourself and explain your role – Tell patient you would like to ask him/her some questions about his/her medication use – Ask if this is a good time • If not, schedule another time

• Ask questions until you are confident all information is complete and reliable – Pursue unclear answers until they are clarified • Use open-ended questions (what, how, why, when) balanced with yes/no questions WHAT medication do you take? Ramipril WHAT is the strength of the Ramipril? 10 mg HOW often do you take it? Once daily WHEN do you take your Ramipril each day? Lunch time Do you ever forget to take your Ramipril? No

• Use nonbiased questions – Do not lead the patient into answering something that may not be true WHAT NOT TO DO So you are taking Ramipril? Yes …and your Ramipril is a 10 mg capsule? Yes …and the Pharmanet record says you take it once daily? Yes …and you take this with your other meds in the morning? Yes …and you are taking routinely without forgetting a dose? Yes

• Ask simple questions – Avoid using medical jargon Are you taking any OTC meds? Are you taking any non-prescription medications? Do you take your lorazepam orally or sublingually? Do you swallow your lorazepam whole or do you place it under your tongue?

• Prompt the patient to remember all medications – Prescriptions • Patches, creams, eye drops, inhalers, sample medications – Over-the-counter (OTC) medications – Herbal and other natural remedies – Vitamins and minerals • Use “head-to-toe” Review of Systems approach

• HEENT – – – Nose, ear or eye drops Analgesics used for headache or sinus pain Dental products Insomnia Motion sickness Smoking Cessation aids • Cardiovascular – Once Daily ASA • Respiratory tract – Antihistamines – Decongestants

• GI/GU – – – Antacids Antiflatulants Antidiarrheals Laxatives Hemorrhoidal preparations Vaginal antiinfectives • Musculoskeletal – ASA – Anti-inflammatory agents – Acetaminophen or combination

• Dermatological – – Psoriatic/Seborrheic Antiinfective Analgesic topical preparation Corns/callus pads or other foot care • Hematological – Consider iron, B 12, folic acid • Overall/System-wide – Vitamins – Herbal – Homeopathic or other alternative healthcare products

• Indication – This is the patient’s version of the indication • Efficacy – Tell me how you know this medication is working for you? • Toxicity – Are there any problems that you are having which you think may be caused by this medication? – If patient says no, probe with a few of the most common side effects

• Compliance – How often do you take this medication? – Try to verify if cost, dosing frequency, adverse effects, or personal beliefs may be an obstacle • How do you feel your medications impact your life? • Tell me how you feel about medication use, in general? – Inquire about technique and maintenance of devices used to facilitate drug delivery or monitor drug therapy • Inhalers and Spacers, BP monitors, Blood glucose monitors

Case Study: Carol Harrison • Interview Carol and document the medication history on the blank Medication History sheet • Use Carol’s Pharmanet record and prescription vials to guide your questions

 Penicillin – Hives Peanuts – Anaphylaxis Ibuprofen – GI upset Eggs?")
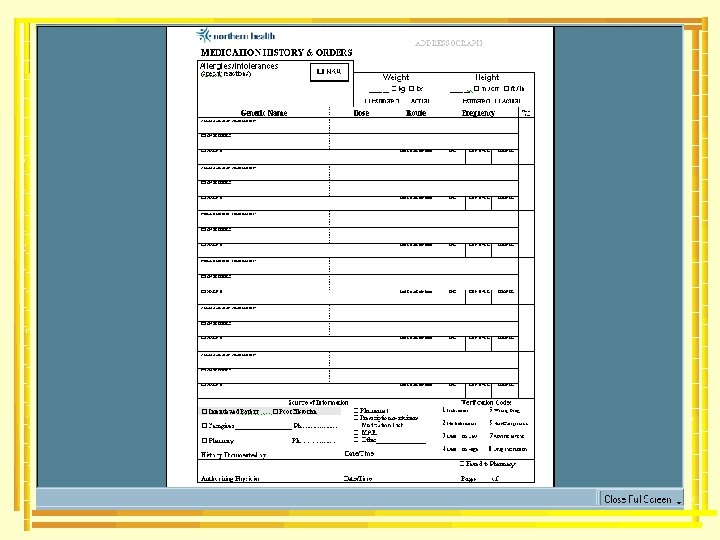
Allergies/Intolerances (specify reactions) Penicillin – Hives Peanuts – Anaphylaxis Ibuprofen – GI upset Eggs? - Rxn Unknown NKA • • • Weight Height ______ kg lbs ______ m / cm ft / in Estimated Actual True Allergy – Drug, food, additives, etc – Immunologically mediated reaction • Type I – Type IV (see Coombs & Gell Classification) Possible Allergy – Vague/incomplete history of allergic reaction – Assume worst case scenario – Include “? ” Intolerance – Side effects or adverse events – Predictable response • N&V, GI upset
 Penicillin – Hives Peanuts – Anaphylaxis Ibuprofen – GI upset Eggs?")
Allergies/Intolerances (specify reactions) Penicillin – Hives Peanuts – Anaphylaxis Ibuprofen – GI upset Eggs? - Rxn Unknown NKA Weight 76. 8___ kg lbs __ Estimated Actual Height ______ m / cm ft / in Estimated Actual • Medication dosing is frequently dependent on weight • Document patient’s weight in kilograms (kg) or pound (lbs) – Actual • Hospital weigh scale – Estimate • Patient report • Nursing estimation
 Penicillin – Hives Peanuts – Anaphylaxis Ibuprofen – GI upset Eggs?")
Allergies/Intolerances (specify reactions) Penicillin – Hives Peanuts – Anaphylaxis Ibuprofen – GI upset Eggs? - Rxn Unknown NKA Weight Height 76. 8___ kg lbs __ Estimated Actual 5’ 6’’_ m / cm ft / in _ Estimated Actual • Some medications require the patient’s height as well • Document patient’s height in either m/cm or ft/in • Only use actual if patient’s height is measured by a healthcare professional at the time of admission

Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate CHANGE ORDER COMMENTS Dose Route Floor Use Frequency Last Dose Date/Time D/C CONTINUE CHANGE • MEDICATION NAME – Document generic name - chemical name of drug • If two chemical ingredients, list both – Avoid use of brand names • Exception: multi-ingredient drugs – Sofracort – framycetin/gramicidin/dexamethasone – Include full name (Erythromycin base, Erythromycin estolate) – Avoid use of abbreviations • Exception: ASA - Acetylsalicylic acid

Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate suspension CHANGE ORDER COMMENTS Dose Route Floor Use Frequency Last Dose Date/Time D/C CONTINUE CHANGE • FORMULATION – Acceptable to use abbreviations • Dosage forms – Susp or Liq - suspension or liquid – Tab or Cap – tablet or capsule • Special formulations – EC – enteric coated – SR – sustained release

Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate suspension CHANGE ORDER Dose 500 mg/ Route Floor Use Frequency 125 mg(5 ml) COMMENTS Last Dose Date/Time D/C CONTINUE CHANGE • DOSE – Weight • mg = milligram, g = gram, mcg = microgram – Do not use µg – confused with mg – Volume • ml = millilitres, L = litres – Miscellaneous • units – Do not use U or u – confused as zero • International Units – Do not use IU – confused with IV or 10 (ten)
")
Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate suspension CHANGE ORDER Dose 500 mg/ 125 mg(5 ml) COMMENTS Route Floor Use Frequency PO Last Dose Date/Time D/C CONTINUE CHANGE • Route – – – po – oral ng – nasogastric sc – subcutaneous im – intramuscular iv – intravenous
")
Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate suspension CHANGE ORDER Dose 500 mg/ 125 mg(5 ml) COMMENTS Route Floor Use Frequency PO TID Last Dose Date/Time D/C CONTINUE CHANGE • FREQUENCY – daily • Do not use q. d. or QD – q 2 days • Do not use q. o. d. or QOD – BID, TID, QID – q 4 h, q 6 h, q 8 h – 5 times daily
")
Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate suspension CHANGE ORDER Dose 500 mg/ 125 mg(5 ml) COMMENTS 2 days of 7 days completed Route Floor Use Frequency PO TID Last Dose Date/Time D/C CONTINUE CHANGE • Duration – If patient has been on medication < 3 months, use comment section to document this information • wks, mths, days, doses… – If medication ordered for specific duration • Indicate time taken in relation to prescribed duration in comment section – 2 doses of 14 days
")
Generic Name PRE-ADMISSION MEDICATION Amoxicillin/Clavulanate suspension CHANGE ORDER Dose 500 mg/ 125 mg(5 ml) COMMENTS Route PO TID Last Dose Date/Time Acute Sinusitis Non-compliance: taking bid 2 days of 7 days completed Floor Use Frequency D/C CONTINUE CHANGE • Comments – Indication as reported by patient if known – Adverse events experienced? – Physician directed patient to reduce dose at last office visit – Non-compliance
")
Generic Name Dose Route Floor Use Frequency PRE-ADMISSION MEDICATION Ranitidine 75 mg tablets (Zantac) CHANGE ORDER 150 mg PO DAILY PRN COMMENTS used occasionally to treat heartburn 6 episodes/mth Last Dose Date/Time Not taken in past week D/C CONTINUE CHANGE • Last dose (date/time) – Documentation not necessary if patient is already receiving treatment in hospital – Helpful in cases where patient uses a medication prn and has not used the medication in the past week – Use 24 hr hospital time – Month and day is adequate

Generic Name Dose PRE-ADMISSION MEDICATION Ibuprofen CHANGE ORDER 400 mg COMMENTS Headaches 1 -2 episodes/month Route Floor Use Frequency PO TID PRN Last Dose Date/Time 1200 hr Sep 12 D/C CONTINUE CHANGE SPECIAL SITUATIONS • Documenting PRN’s – Record frequency if there is a pattern – Include indication and frequency of episodes – Record in “Last Dose” column if medication not taken in past week

Generic Name PRE-ADMISSION MEDICATION Etidronate 400 mg/Calcium 1250 mg Kit CHANGE ORDER COMMENTS Osteoporosis 56 tablets left in 90 day kit Dose 1 tab Route Floor Use Frequency PO Daily Last Dose Date/Time 0800 hr Sep 12 D/C CONTINUE CHANGE SPECIAL SITUATIONS • Medications given in cycles – Didrocal kit – note where patient is in 90 day cycle
 PRE-ADMISSION MEDICATION Cyanocobalamin CHANGE ORDER COMMENTS")
Generic Name Dose 1, 000 mcg (1 ml) PRE-ADMISSION MEDICATION Cyanocobalamin CHANGE ORDER COMMENTS Anemia Next dose due: Oct 21 Route Floor Use Frequency IM Monthly Last Dose Date/Time 0800 hr Sep 21 D/C CONTINUE CHANGE • SPECIAL SITUATION – Medications given at intervals • Note due date of next dose as well as last dose

Source of Information Verification Codes Interviewed Patient Poor Historian 1 Indication 5 Wrong Drug Pharmanet 2 No Indication 6 Non-Compliance Prescription containers Caregiver _ Jane Smith_ Ph: 987 -4321 Medication List Wal-Mart _ Ph: 987 -6543 3 Dose Too Low 7 Adverse Event MAR Pharmacy _ 4 Dose Too High 8 Drug Interaction Other________ History Documented by Date/Time • Indicate Source of Information – Ideal to interview patient • Limitations if patient: – Confused – Does not speak English – Too ill to interview – A good idea to document Pharmacy and Caregiver contact info in the event more information is needed later

Source of Information Verification Codes Interviewed Patient Poor Historian Pharmanet 1 Indication 5 Wrong Drug 2 No Indication 6 Non-Compliance Prescription containers Caregiver _ Jane Smith_ Ph: 987 -4321 Medication List Wal-Mart _ Ph: 987 -6543 MAR Pharmacy _ Other________ History Documented by Alana Froese Date/Time Today’s Date • Sign your name • Record date and time 3 Dose Too Low 7 Adverse Event 4 Dose Too High 8 Drug Interaction

Case Study: Evelyn Smith • Use the new Medication History worksheet to interview Evelyn Smith • Evelyn was admitted to Emergency with mild confusion and dehydration • She has not brought in her prescription vials however, you have printed her Pharmanet record in preparation for the interview


• Access the patient’s chart to compare admission orders to the medication history documented • Look in history or progress note sections of patient chart for reason for any changes • You are going to be shown how you can use this information to identify and document discrepancies


• Type 0 - No Discrepancy • Type 1 - Intentional • Physician has made an intentional choice to add, change, discontinue a medication • Choice is clearly documented • Type 2 - Undocumented Intentional • Physician has made an intentional choice to add, change, discontinue a medication • Choice is not clearly documented • Type 3 - Unintentional • Physician unintentionally changed, added, or omitted a medication the patient was taking prior to admission

• Purpose – A quick method used to indicate physician’s reason for continuing, changing or discontinuing a pre-admission medication Verification Codes 1 Indication 5 Wrong Drug 2 No Indication 6 Non-Compliance 3 Dose Too Low 7 Adverse Event 4 Dose Too High 8 Drug Interaction

• INDICATION 1. Patient has a diagnosed problem which requires a drug therapy 1. New symptoms or indication revealed/presented 2. Preventative drug required 1. Taking a drug for valid indication, but this drug causes side effects which require prophylactic therapy 3. Synergistic drug required 1. Requires synergistic drug therapy to potentiate effect of current drug therapy

• NO INDICATION ØNo clear indication for drug use ØImprovement of disease state ØReceiving drug chronically which was intended for acute condition ØRecreational use, addiction/dependence ØCondition can be more appropriately treated by non-drug therapy ØReceiving a drug to treat an avoidable ADR ØInappropriate duplication of therapeutic class or active ingredient
 ØDosage regime")
• DOSE TOO LOW/DURATION TOO SHORT ØDrug dose too low (sub-therapeutic) ØDosage regime not frequent enough ØDuration of treatment too short
")
• DOSE TOO HIGH/DURATION TOO LONG ØDrug dose too high (dose dependent toxicity) ØDosage regime too frequent ØDuration of treatment too long

• WRONG DRUG 1. Inappropriate drug or dosage selection 2. More cost effective drug available 3. Drug therapy is known to be ineffective for this indication 4. Drug therapy is effective for this indication, but not effective in this patient for unknown reasons 2. Inappropriate drug form 1. Cannot take the drug product (swallow, taste, administration) 3. Contraindication for drug (incl. pregnancy/ breastfeeding)

• NON-COMPLIANCE Ø Patient is not compliant Ø Drug underused, overused or abused Ø Patient has difficulties reading/understanding Ø Drug not taken/administered at all Ø Patient unable to use drug/form as directed Ø Patient unwilling to carry financial costs Ø Prescribed drug not available Ø Wrong drug taken/administered Ø Prescribing error Ø Dispensing error (wrong drug or dose dispensed) Ø Administration error (by patient/caregivers)
 ØSide effect")
• ADVERSE EVENT ØSide effect suffered at a therapeutic dose (non-allergic) ØSide effect suffered at a therapeutic dose (allergic) ØToxic effects suffered

• DRUG INTERACTION ØPotential or actual Drug/Drug interaction ØPotential or actual Drug/Food interaction ØPotential or actual Drug/Laboratory interaction

Generic Name PRE-ADMISSION MEDICATION Ramipril CHANGE ORDER Dose 10 mg Route Floor Use Frequency PO BID 0 COMMENTS Last Dose Date/Time D/C CONTINUE CHANGE 1 • If there is no change, add the verification code “ 1” to the continue box • Document a Type 0 discrepancy in the “Floor Use” section

Generic Name PRE-ADMISSION MEDICATION Ramipril CHANGE ORDER Ramipril Dose 10 mg 5 mg Route Floor Use Frequency PO BID PO 1 Daily COMMENTS Last Dose Date/Time D/C CONTINUE CHANGE 4 • When there are differences, write the admission order below the medication in question • If a reason for the change has been documented by the ordering physician, use one of the verification codes to indicate the intention of the change • Document a Type 1 discrepancy in the “Floor Use” section

Generic Name PRE-ADMISSION MEDICATION Hydrochlorothiazide CHANGE ORDER Hydrochlorothiazide Dose 25 mg 12. 5 mg Route Floor Use Frequency PO QAM PO ? QAM COMMENTS Last Dose Date/Time D/C CONTINUE CHANGE ? • If a reason for the change has NOT been documented by the ordering physician, this discrepancy may either be a Type 2 or Type 3 discrepancy • Clarification with the ordering physician will be required before the type of the discrepancy can be documented • In this case, leave “undocumented” until resolved by the clinical pharmacist

Generic Name PRE-ADMISSION MEDICATION Ramipril CHANGE ORDER Nil COMMENTS Dose 10 mg Route Floor Use Frequency PO BID 1 Last Dose Date/Time D/C 7 CONTINUE CHANGE • When there are no matching admission orders, write “nil” below the medication in question • If a reason for the discontinuation has been documented by the ordering physician, use one of the verification codes to indicate the intention to stop • Document a Type 1 discrepancy in the “Floor Use” section

Generic Name PRE-ADMISSION MEDICATION Ramipril CHANGE ORDER Nil COMMENTS Dose 10 mg Route Floor Use Frequency PO BID ? Last Dose Date/Time D/C ? CONTINUE CHANGE • If a reason for the discontinuation has NOT been documented by the ordering physician, this discrepancy may either be a Type 2 or Type 3 discrepancy • Clarification with the ordering physician will be required before the type of the discrepancy can be documented • In this case, leave “undocumented” until resolved by the clinical pharmacist

Case Study: Evelyn Smith • You have been to Evelyn’s chart and have reviewed the admission orders – See physician order sheet provided to you • The only place in the chart you could find explanations for changes to pre-admission medications is on the actual physician order sheet. • Begin the reconciliation process by comparing the medication history to the admission medications ordered and filling out the second part of the Medication History form


• All potential type 2 or 3 discrepancies are to be documented on the Discrepancy Clarification & Resolution Form • Addressograph the form • Transcribe all information collected on potential type 2 or 3 discrepancies onto this second form • Document sources of information • Include signature and date under source of information section • Direct both forms to the Clinical Pharmacist for review and clarification/resolution

• After reviewing and assessing level of urgency to resolve, the pharmacist may choose to either: • Place the form on the patient’s chart to be completed by the physician OR • Calling the physician for clarification and writing verbal orders onto the form then placing the form onto the patient’s chart for processing OR • Using the form as a worksheet only and, after clarifying, writing the verbal orders into the patient’s chart

Generic Name PRE-ADMISSION MEDICATION Hydrochlorothiazide ORDER AT ADMISSION Hydrochlorothiazide COMMENTS Hypertension Dose 25 mg 12. 5 mg Route PO PO Frequency Continue admission order QAM Revert to pre-admission order • If the physician states he/she intended to change the order but did not document this on the patient’s chart, the physician/pharmacist will indicate “Continue Admission Order” Floor Use

Generic Name PRE-ADMISSION MEDICATION Ramipril ORDER AT ADMISSION Nil COMMENTS Hypertension Dose 10 mg Route PO Frequency BID Continue admission order Revert to pre-admission order • If the physician states he/she DID NOT intend to change the order, the physician/pharmacist will indicate “Revert to Pre-Admission Order” Floor Use

Discrepancy Types Source of Information Undocumented Intentional Resolution: Continue admission order Interviewed Patient Poor Historian Caregiver _ Jane Smith_ Ph: 987 -4321 Pharmacy _ Wal-Mart _ Ph: 987 -6543 History Documented by Nancy Green Pharmanet Prescription containers Medication List MAR Other________ Date/Time Unintentional Resolution: Revert to pre- admission order Today’s Date v/o Dr. B. Brown/Alana Froese Date/Time Today’s Date Authorizing Physician Faxed to Pharmacy Pages ____ of ____ • Physician/Pharmacist to sign and date at bottom of form • Ideally, to be placed in patient’s chart and processed as an order

Case Study: Evelyn Smith • Complete a Discrepancy Clarification & Resolution form – Ensure all potential type 2 & 3 discrepancies are filled in on the form – Refer this form as well as your original Medication History to your pharmacist for review – In this case, the pharmacist determined the physician should be called to clarify discrepancies – Call physician and document clarifications on Discrepancy Clarification & Resolution form


Generic Name PRE-ADMISSION MEDICATION Hydrochlorothiazide CHANGE ORDER Dose 25 mg Hydrochlorothiazide 12. 5 mg Route Floor Use Frequency PO QAM PO 2 QAM COMMENTS Last Dose Date/Time D/C CONTINUE CHANGE 4 • BACK TO THE MEDICATION HISTORY WORKSHEET… • A member of the Clinical Pharmacy team will indicate the reason for an undocumented intended change once clarified • Place a verification code in the change box • In this case, a Type 2 discrepancy is documented in the Floor Use box

Generic Name PRE-ADMISSION MEDICATION Ramipril CHANGE ORDER Nil COMMENTS Dose 10 mg Route Floor Use Frequency PO BID 3 Last Dose Date/Time D/C CONTINUE CHANGE 1 • If an Unintentional Discrepancy is identified • Indicate a Type 3 discrepancy in the Floor Use box • In this situation, the physician reverted to the preadmission order indicating a true error occurred

Dr. B. Brown/Alana Froese Date/Time Today’s Date Authorizing Physician Faxed to Pharmacy Pages __1__ of __1__ • The person who completes the resolution information must indicate the physician who was involved and sign/date the bottom of the form • As this is considered a worksheet only, the Faxed to Pharmacy section is not used and this form is not processed as an order • The Pharmacy Technician will be responsible for maintaining all forms, compiling statistics and generating monthly discrepancy reports

Case Study: Evelyn Smith – The final step! – Document resolutions on Medication History form – Return to Technician to compile statistics


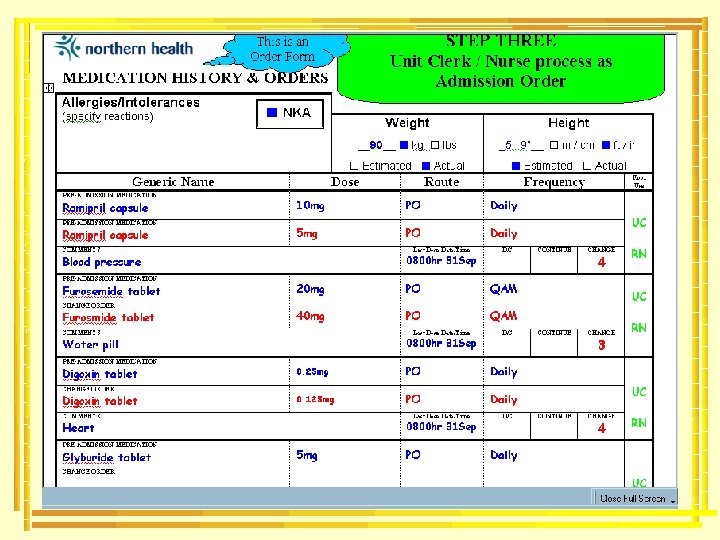
Generic Name PRE-ADMISSION MEDICATION Ramipril ORDER AT ADMISSION Nil Dose 10 mg Route PO Frequency BID Floor Use UC RN COMMENTS Hypertension Continue admission order Revert to pre-admission order • Unit Clerk/Nurse will transcribe orders to MAR and initial in Floor Use section • RN will check orders and accuracy of transcription and will initial below the first initials in the Floor Use section

Discrepancy Types Source of Information Undocumented Intentional Resolution: Continue admission order Interviewed Patient Poor Historian Caregiver _ Jane Smith_ Ph: 987 -4321 Pharmacy _ Pharmanet Prescription containers Medication List MAR Other________ Unintentional Resolution: Revert to pre- admission order Wal-Mart _ Ph: 987 -6543 History Documented by Nancy Green Date/Time Today’s Date Faxed to Pharmacy v/o Dr. B. Brown/Alana Froese Date/Time Today’s Date Authorizing Physician 1 1 Pages __ ___ of __ ___ • Unit Clerk/Nurse will indicate number of pages & check Faxed to Pharmacy Box when sending to pharmacy

Case Study: Carol Harrison • You have just completed a BPMH 1. Compare the Physician Orders to the Medication History 1. 2. 3. 4. 5. Note: you are unable to glean additional information regarding the rational to therapeutic changes from other sections in the chart Document Discrepancies on Medication History form Complete Discrepancy Clarification & Resolution (DCR) form Call physician to clarify discrepancies and document on DCR form Document resolution of discrepancies on Medication History form

An accurate medication history is performed prior to physician admission order writing This history is used to write admission orders PREVENTS ERRORS

Nurse/Physician/Pharmacy use Medication History & Orders Form to document medication history Physician uses Medication History & Orders Form to indicate continuation, discontinuation or change to pre-admission medications. Any others admission orders are written on usual physician order sheet Orders are processed to pharmacy using Medication History & Orders Form for any preadmit medications and using the physician’s order sheet for any new admission orders

“The names of the patients whose lives we save can never be known. Our contribution will be what did not happen to them. And, though they are unknown, we will know that mothers and fathers are at graduations and weddings they would have missed, and that grandchildren will know grandparents they might never have known, and holidays will be taken, and work completed, and books read, and symphonies heard, and gardens tended that, without our work, would never have been. ” Donald M. Berwick, MD, MPP President and CEO Institute for Healthcare Improvement
55067369c3cf2bf0a91d39063fca5630.ppt