62a1f33f5c3c71f1154f8f7f110740de.ppt
- Количество слайдов: 57



1 Transmission and Pathogenesis of Tuberculosis 1
 2. Explain how")
Module 1: Objectives 1. Briefly describe the history of tuberculosis (TB) 2. Explain how TB is spread (transmission) 3. Explain the difference between latent TB infection (LTBI) and TB disease 4. Explain how LTBI and TB disease develop (pathogenesis) 5. Describe the classification system for TB Module 1 – Transmission and Pathogenesis of Tuberculosis 2

History of TB 3
 • TB has affected humans for millennia • Historically known")
History of TB (1) • TB has affected humans for millennia • Historically known by a variety of names, including: – Consumption – Wasting disease – White plague • TB was a death sentence for many Vintage image circa 1919 Image credit: National Library of Medicine Module 1 – Transmission and Pathogenesis of Tuberculosis 4
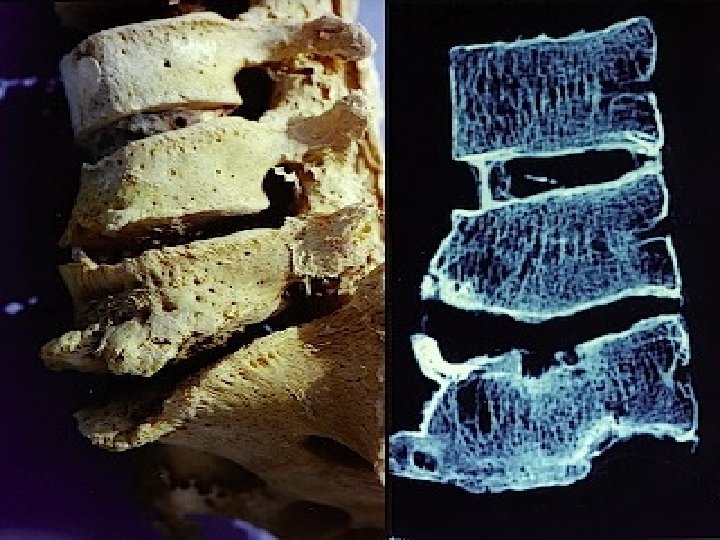

HISTORY • Bone lesions in mummified skeletons since 1, 000 BC • Hippocrates - term “phthisis” meaning consumption • “ Tuberculosis” comes from tubercules (fr. )- describing the clinical lesions • Middle Ages- “White Plague” – having TB was the equivalent of a death sentence • 1882 – 24 th March- the German pathologist Robert Koch identified the TB bacillus Mycobacterium tuberculosis • 1907 - Development of the first vaccine “BCG” • 1944 – Chemotherapy using the single antibiotic to treat active TB • 1950 s – Multiple drug chemotherapy

ROBERT KOCH 1882
 Scientific Discoveries in 1800 s • Until mid-1800 s, many")
History of TB (2) Scientific Discoveries in 1800 s • Until mid-1800 s, many believed TB was hereditary • 1865 Jean Antoine. Villemin proved TB was contagious • 1882 Robert Koch discovered M. tuberculosis, the bacterium that causes TB Mycobacterium tuberculosis Image credit: Janice Haney Carr Module 1 – Transmission and Pathogenesis of Tuberculosis 8
 Sanatoriums • Before TB antibiotics, many patients were sent to")
History of TB (3) Sanatoriums • Before TB antibiotics, many patients were sent to sanatoriums • Patients followed a regimen of bed rest, open air, and sunshine • TB patients who could not afford sanatoriums often died at home Sanatorium patients resting outside Module 1 – Transmission and Pathogenesis of Tuberculosis 9

Nobel Prizes for Medicine… “is awarded to those who have conferred the greatest benefit of mankind in the field of medicine” 1882 – dr. Robert Koch – discovery of the TB bacillus 1908 – dr. Paul Ehrlich – use of drugs to combat infection 1939 – dr. Gerhard Domagk – discovery of first anti – TB drug Prontosil 1952 – dr. Selman Waksman – development of SM as a drug cure for TB
, isoniazid (1952), pyrazinamide (1954), cycloserine (1955),")
TB MEDICATION • • • p-aminosalicylic acid (1946), isoniazid (1952), pyrazinamide (1954), cycloserine (1955), ethambutol (1962) rifampicin (1963)

Breakthrough in the Fight Against TB • After 1960, TB death rates began to drop dramatically • Each year, fewer people got TB • Many TB sanatoriums had closed by mid 1980 s Module 1 – Transmission and Pathogenesis of Tuberculosis 12

TB Resurgence • Increase in TB in mid 1980 s • Contributing factors: – Inadequate funding for TB control programs – HIV epidemic – Increased immigration from countries where TB is common – Spread in homeless shelters and correctional facilities – Increase and spread of multidrug-resistant TB March 16, 1992 Newsweek Magazine Cover Module 1 – Transmission and Pathogenesis of Tuberculosis 13

TB History Timeline 1993: TB cases decline due to increased funding and enhanced TB control efforts 1865: Jean. Antoine Villemin proved TB is contagious 1840 1860 1884: First TB sanatorium established in U. S. 1880 1900 1882: Robert Koch discovers M. tuberculosis 1943: Streptomycin (SM) a drug used to treat TB is discovered Mid-1970 s: Most TB sanatoriums in U. S. closed 1920 1960 1943 -1952: Two more drugs are discovered to treat TB: INH and PAS 1980 2000 Mid-1980 s: Unexpected rise in TB cases Module 1 – Transmission and Pathogenesis of Tuberculosis 14

TB Transmission 15
 Transmission is defined as the spread of an organism, such as")
TB Transmission (1) Transmission is defined as the spread of an organism, such as M. tuberculosis, from one person to another. Module 1 – Transmission and Pathogenesis of Tuberculosis 16
 Types of Mycobacteria • M. tuberculosis causes most TB cases •")
TB Transmission (2) Types of Mycobacteria • M. tuberculosis causes most TB cases • Mycobacteria that cause TB: – – – M. tuberculosis M. bovis M. africanum M. microti M. canetti • Mycobacteria that do not cause TB M. tuberculosis – M. avium complex, M. xenopi, M. Kansasi Module 1 – Transmission and Pathogenesis of Tuberculosis 17
 • Since TB is a disease of respiratory transmission, optimal conditions")
TB Transmission (3) • Since TB is a disease of respiratory transmission, optimal conditions for transmission include: – overcrowding – poor personal hygiene – poor public hygiene
 • TB is spread person to person through the air via")
TB Transmission (4) • TB is spread person to person through the air via droplet nuclei • M. tuberculosis may be expelled when an infectious person: – – Coughs Sneezes Speaks Sings • Transmission occurs when another person inhales droplet nuclei Module 1 – Transmission and Pathogenesis of Tuberculosis 19
 Dots in air represent droplet nuclei containing M. tuberculosis Module 1")
TB Transmission (5) Dots in air represent droplet nuclei containing M. tuberculosis Module 1 – Transmission and Pathogenesis of Tuberculosis 20
 • Probability that TB will be transmitted depends on: – Infectiousness")
TB Transmission (6) • Probability that TB will be transmitted depends on: – Infectiousness of person with TB disease – Environment in which exposure occurred – Length of exposure – Virulence (strength) of the tubercle bacilli • The best way to stop transmission is to: – Isolate infectious persons – Provide effective treatment to infectious persons as soon as possible Module 1 – Transmission and Pathogenesis of Tuberculosis 21

MYCOBACTERIUM TUBERCULOSIS • is the etiologic agent of tuberculosis in humans. • is a fairly large nonmotile rod-shaped bacterium • is an obligate aerobe • is a facultative intracellular parasite • has a slow generation time

Mycobacterium tuberculosis • serpentine cords not classified as either Gram-positive or Gramnegative • acid-fast bacteria resist de staining by acid-alcohol after being stained by certain Mycobacterium aniline dyes tuberculosis. Acid-fast stain (Ziehl Neelsen)

Mycobacterium tuberculosis • Impermeability to stains and dyes • Resistance to many antibiotics • Resistance to killing by acidic and alkaline compounds • Resistance to osmotic lysis via complement deposition • Resistance to lethal oxidations and survival inside of macrophages

The cell wall structure of Mt • There is no true outer membrane in M. Tuberculosis • The cell wall complex contains peptidoglycan, arabinogalactan and mycolic acid and lipoarabinomannan. • Over 60% of the mycobacterial cell wall is lipid – Mycolic acid – 50% of the dry weight of the cell wall • It is strong hydrophobic • Considered an important determinant of virulence

Growth characteristics • Very slow growth rate – generation time of 20 - 24 hrs • Grow on simple carbon and inorganic nitrogen sources • Rough, non-pigmented corded colonies, with a weak catalase activity and reduces nitrate Types of media: • Albumin in an agar base – Lowenstein-Jensen • Potato and egg base media- Middlebrock - Broth based culture systems for improvement in speed and sensitivity – – BACTEC MGIT Septi Check AFB CAMLIC ( Continuosly Automated Mycobacterial Liquid Culture system)

Mycobacterium tuberculosis • Has a particular predilection for the lungs • Has special mechanisms for cell entry. • Can grow intracellularly • Interferes with the toxic effects of reactive oxygen

VIRULENCE MECHANISMS AND FACTORS common for nearly all mycobacteria • Mycolic acid glicolipids can elicit granuloma formation • Catalase-peroxidase - resist the host cell oxidative response • Sulfatides and trehalose dimycolate - trigger toxicity in animal models

Mycobacterium tuberculosis Inhalation and deposition in the lungs of the bacillus leads to: • Clearance of the organism or • latent infection or • Rapid progressive disease (primary disease) • Active disease many years after the infection (reactivation disease)

TB Pathogenesis 30
 Pathogenesis is defined as how an infection or disease develops in")
TB Pathogenesis (1) Pathogenesis is defined as how an infection or disease develops in the body. Module 1 – Transmission and Pathogenesis of Tuberculosis 31
 Latent TB Infection (LTBI) • Occurs when tubercle bacilli are in")
TB Pathogenesis (2) Latent TB Infection (LTBI) • Occurs when tubercle bacilli are in the body, but the immune system is keeping them under control • Detected by the Mantoux tuberculin skin test (TST) or by blood tests such as interferongamma release assays (IGRAs) which include: – Quanti. FERON®-TB Gold test (QFT-G) – Quanti. FERON®-TB Gold In-Tube (QFT-GIT) – T-Spot®. TB test (T-SPOT) • People with LTBI are NOT infectious Module 1 – Transmission and Pathogenesis of Tuberculosis 32
 TB Disease • Develops when immune system cannot keep tubercle bacilli")
TB Pathogenesis (3) TB Disease • Develops when immune system cannot keep tubercle bacilli under control – May develop very soon after infection or many years after infection • About 10% of all people with normal immune systems who have LTBI will develop TB disease at some point in their lives • People with TB disease are often infectious Module 1 – Transmission and Pathogenesis of Tuberculosis 33
 Droplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and")
TB Pathogenesis (4) Droplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and travel to alveoli Module 1 – Transmission and Pathogenesis of Tuberculosis 34
 Tubercle bacilli multiply in alveoli, where infection begins Module 1 –")
TB Pathogenesis (5) Tubercle bacilli multiply in alveoli, where infection begins Module 1 – Transmission and Pathogenesis of Tuberculosis 35
 A small number of tubercle bacilli enter bloodstream and spread throughout")
TB Pathogenesis (6) A small number of tubercle bacilli enter bloodstream and spread throughout body Module 1 – Transmission and Pathogenesis of Tuberculosis 36
 LTBI • Within 2 to 8 weeks the immune system produces")
TB Pathogenesis (7) LTBI • Within 2 to 8 weeks the immune system produces immune cells (macrophages, T lymphocytes, giant cells, epithelioid cells) that surround the tubercle bacilli • These cells form a barrier shell that keeps the bacilli contained and under control (LTBI) Module 1 – Transmission and Pathogenesis of Tuberculosis 37
 TB Disease • If the immune system CANNOT keep tubercle bacilli")
TB Pathogenesis (8) TB Disease • If the immune system CANNOT keep tubercle bacilli under control, bacilli begin to multiply rapidly and cause TB disease • This process can occur in different places in the body Module 1 – Transmission and Pathogenesis of Tuberculosis 38
 • Droplet nuclei are inhaled and need to reach")
Stages of TB pathogenesis (1) • Droplet nuclei are inhaled and need to reach the alveolar space. • 7 -21 days after initial infection – mycobact tuberculosis multiplies within macrophages until the macrophages burst. • Then: – T cells become activated and liberate cytokines, including gamma interferon – the individual becomes tuberculin-positive – activated macrophages may release lytic enzymes and cytokines – tubercle formation begins
 • This is known as the primary infection. The")
Stages of TB pathogenesis (2) • This is known as the primary infection. The patient will heal and a scar will appear in the infected sites. There will also be a few viable bacilli/spores may remain in these areas (particularly in the lung). The bacteria at this time goes into a dormant state, as long as the person's immune system remains active and functions normally this person isn't bothered by the dormant bacillus. • When a person's immune system is depressed. , a secondary reactivation occurs. • 85 -90% of the cases seen which are of secondary reactivation type occur in the lungs.
 When a person's immune system is weak, • Progressive")
Stages of TB pathogenesis (3) When a person's immune system is weak, • Progressive destruction occurs: bacterial products, tumor necrosis factor, reactive oxygen intermediates and reactive nitrogen intermediates, contents of cytotoxic cells • caseous necrosis • Bacilli may spread hematogenously to produce disseminated TB • Bacilli may spread mechanically into lung airways!

Untreated • 80% will die • Recover • Chronic disease – repeated episodes of spontan healing by fibrotic changes around the lessions • Reactivation disease – persistent bacteria suddenly proliferate – disease process is localized, lesion located at the lung apices, with less dissemination
 TB Disease (in the lungs) Inactive,")
LTBI vs. TB Disease Latent TB Infection (LTBI) TB Disease (in the lungs) Inactive, contained tubercle bacilli Active, multiplying tubercle bacilli in the body TST or blood test results usually positive Chest x-ray usually normal Chest x-ray usually abnormal Sputum smears and cultures negative Sputum smears and cultures may be positive No symptoms Symptoms such as cough, fever, weight loss Not infectious Often infectious before treatment Not a case of TB A case of TB Module 1 – Transmission and Pathogenesis of Tuberculosis 43

TB Pathogenesis Progression from LTBI to TB Disease 44
 • Risk of developing TB disease is highest the")
Progression to TB Disease (1) • Risk of developing TB disease is highest the first 2 years after infection • People with LTBI can be given treatment to prevent them from developing TB disease • Detecting TB infection early and providing treatment helps prevent new cases of TB disease Module 1 – Transmission and Pathogenesis of Tuberculosis 45
 Some conditions increase probability of LTBI progressing to TB")
Progression to TB Disease (2) Some conditions increase probability of LTBI progressing to TB disease • Infection with HIV • Organ transplant • Chest x-ray findings suggestive of previous TB • Silicosis • Substance abuse • Recent TB infection • Diabetes mellitus • Severe kidney disease • Certain types of cancer • Prolonged therapy with corticosteroids and other immunosuppressive therapy, • Certain intestinal conditions such as prednisone and • Low body weight tumor necrosis factor-alpha [TNF-α] antagonists Module 1 – Transmission and Pathogenesis of Tuberculosis 46
 People Exposed to TB Not TB Infected Latent TB")
Progression to TB Disease (3) People Exposed to TB Not TB Infected Latent TB Infection (LTBI) Not Infectious Negative TST or QFT-G test result Positive TST or QFT-G test result No TB Infection Figure 1. 5 Latent TB Infection May go on to develop TB disease Module 1 – Transmission and Pathogenesis of Tuberculosis 47
 TB and HIV In an HIV-infected person, TB can")
Progression to TB Disease (4) TB and HIV In an HIV-infected person, TB can develop in one of two ways: • Person with LTBI becomes infected with HIV and then develops TB disease as the immune system is weakened • Person with HIV infection becomes infected with M. tuberculosis and then rapidly develops TB disease Image credit: Mississippi State Department of Health Module 1 – Transmission and Pathogenesis of Tuberculosis 48
 TB and HIV People who are infected with both")
Progression to TB Disease (5) TB and HIV People who are infected with both M. tuberculosis and HIV are much more likely to develop TB disease TB infection and NO risk factors TB infection and HIV infection (pre-Highly Active Antiretroviral Treatment [HAART]) Risk is about 5% in the first 2 years after infection and about 10% over a lifetime Risk is about 7% to 10% PER YEAR, a very high risk over a lifetime Module 1 – Transmission and Pathogenesis of Tuberculosis 49

TB Pathogenesis Sites of TB Disease 50
 Bacilli may reach any part of the body, but")
Sites of TB Disease (1) Bacilli may reach any part of the body, but common sites include: Module 1 – Transmission and Pathogenesis of Tuberculosis 51
 Location Pulmonary TB Lungs Extrapulmonary TB Places other than")
Sites of TB Disease (2) Location Pulmonary TB Lungs Extrapulmonary TB Places other than lungs such as: • Larynx • Lymph nodes • Pleura • Brain • Kidneys • Bones and joints Miliary TB Carried to all parts of body, through bloodstream Frequency Most TB cases are pulmonary Found more often in: • HIV-infected or other immunosuppressed persons • Young children Rare Module 1 – Transmission and Pathogenesis of Tuberculosis 52

TB Pathogenesis TB Classification System 53
 Based on pathogenesis of TB Class Type Description 0 No")
TB Classification System (1) Based on pathogenesis of TB Class Type Description 0 No TB exposure Not infected No history of TB exposure Negative result to a TST or IGRA 1 TB exposure No evidence of infection History of TB exposure Negative result to a TST (given at least 810 weeks after exposure) or IGRA 2 TB infection No TB disease Positive result to a TST or IGRA Negative smears and cultures (if done) No clinical or x-ray evidence of active TB disease Module 1 – Transmission and Pathogenesis of Tuberculosis 54
 Based on pathogenesis of TB Class Type Description 3 TB,")
TB Classification System (2) Based on pathogenesis of TB Class Type Description 3 TB, clinically active Positive culture (if done) for M. tuberculosis Positive result to a TST or IGRA, and clinical, bacteriological, or x-ray evidence of TB disease 4 Previous TB disease (not clinically active) Medical history of TB disease Abnormal but stable x-ray findings Positive result to a TST or IGRA Negative smears and cultures (if done) No clinical or x-ray evidence of active TB disease 5 TB suspected Signs and symptoms of TB disease, but evaluation not complete Module 1 – Transmission and Pathogenesis of Tuberculosis 55
 A 30 -year-old man visits the health department for")
Module 1: Case Study (1) A 30 -year-old man visits the health department for a TST because he is required to have one before starting his new job as a health care worker. He has an 18 mm positive reaction to the TST. He has no symptoms of TB, and his chest x-ray findings are normal. (pg. 16) Module 1 – Transmission and Pathogenesis of Tuberculosis 56
 Should this be considered a case of TB? No.")
Module 1: Case Study (2) Should this be considered a case of TB? No. The man described above has TB infection. He has an 18 mm positive reaction to TST, but no evidence of TB disease. Therefore, this is not a case of TB. Should this man be considered infectious? No, he should not be considered infectious. This man has LTBI, not TB disease. People with TB infection and no evidence of TB disease are not infectious. Module 1 – Transmission and Pathogenesis of Tuberculosis 57
62a1f33f5c3c71f1154f8f7f110740de.ppt