

ДС Респирторная поддержка в неонаталогии 103 слайда.pptx
- Количество слайдов: 103
 1 РЕСПИРАТОРНАЯ ПОДДЕРЖКА В НЕОНАТОЛОГИИ
1 РЕСПИРАТОРНАЯ ПОДДЕРЖКА В НЕОНАТОЛОГИИ
 СОВРЕМЕННЫЕ АСПЕКТЫ НЕИНВАЗИВНОЙ РЕСПИРАТОРНОЙ ПОДДЕРЖКИ В НЕОНАТОЛОГИИ 10 ФЕВРАЛЯ 2012 Г. НИЖНИЙ НОВГОРОД V. Chijenas, MD Neonatal Department of Vilnius Maternity Hospital, Lithuania 2
СОВРЕМЕННЫЕ АСПЕКТЫ НЕИНВАЗИВНОЙ РЕСПИРАТОРНОЙ ПОДДЕРЖКИ В НЕОНАТОЛОГИИ 10 ФЕВРАЛЯ 2012 Г. НИЖНИЙ НОВГОРОД V. Chijenas, MD Neonatal Department of Vilnius Maternity Hospital, Lithuania 2
 World Population Growth Per Time Unit Time unit Births Deaths 131, 571, 719 55, 001, 289 76, 570, 430 10, 964, 310 4, 583, 441 6, 380, 869 Day 360, 470 150, 688 209, 782 Hour 15, 020 6, 279 8, 741 Minute 250 105 146 Seconds 4. 2 1. 7 2. 4 Year Month Natural Increase Source: US Census Bureau, International Data Base. (Figures may not add to totals due to rounding)
World Population Growth Per Time Unit Time unit Births Deaths 131, 571, 719 55, 001, 289 76, 570, 430 10, 964, 310 4, 583, 441 6, 380, 869 Day 360, 470 150, 688 209, 782 Hour 15, 020 6, 279 8, 741 Minute 250 105 146 Seconds 4. 2 1. 7 2. 4 Year Month Natural Increase Source: US Census Bureau, International Data Base. (Figures may not add to totals due to rounding)
 Being born preterm In Europe and many developed countries the preterm birth rate is generally 5– 9%, and in the USA it has even risen to 12– 13% in the last decades. Preterm birth is a significant cost factor in healthcare, not even considering the expenses of long-term care for individuals with disabilities due to preterm birth. A 2003 study in the US determined neonatal costs to be $224, 400 for a newborn at 500– 700 g versus $1, 000 at over 3, 000 g By gestational age: 5% of preterm births occur at less than 28 weeks (extreme prematurity), 1 % of all babies (about 13 mln. ) worldwide are born at less than 28 weeks/year. 15% at 28– 31 weeks (severe prematurity), 20% at 32– 33 weeks (moderate prematurity) 60– 70% at 34– 36 weeks (late preterm)
Being born preterm In Europe and many developed countries the preterm birth rate is generally 5– 9%, and in the USA it has even risen to 12– 13% in the last decades. Preterm birth is a significant cost factor in healthcare, not even considering the expenses of long-term care for individuals with disabilities due to preterm birth. A 2003 study in the US determined neonatal costs to be $224, 400 for a newborn at 500– 700 g versus $1, 000 at over 3, 000 g By gestational age: 5% of preterm births occur at less than 28 weeks (extreme prematurity), 1 % of all babies (about 13 mln. ) worldwide are born at less than 28 weeks/year. 15% at 28– 31 weeks (severe prematurity), 20% at 32– 33 weeks (moderate prematurity) 60– 70% at 34– 36 weeks (late preterm)

 K. Bohlin (Karolinska University Hospital, Stockholm) Breath,") C. C. Roehr (Charite University Hospital, Berlin) K. Bohlin (Karolinska University Hospital, Stockholm) Breath, September 2011, Vol. 8, No 1 Частота острых заболевании лёгких у новорожденных около 3% - СДР - транзиторная тахипноэ - Инфекция, пневмония 500 – 1500 g. СДР > 50% 500 – 750 g. СДР – 90%
C. C. Roehr (Charite University Hospital, Berlin) K. Bohlin (Karolinska University Hospital, Stockholm) Breath, September 2011, Vol. 8, No 1 Частота острых заболевании лёгких у новорожденных около 3% - СДР - транзиторная тахипноэ - Инфекция, пневмония 500 – 1500 g. СДР > 50% 500 – 750 g. СДР – 90%
 – самый ранний гестационный возрат при котором шанс") Недоношенность Пределы жизнеспособности (limit of viability) – самый ранний гестационный возрат при котором шанс выживаемости не менее 50%. В развитых странах около 50% новорожденных при гестационном возрате 24 недели выживают. При этом половина из них инвалидизированна. 80% новорожденных, при гестационном возрате 28 недель, выживают без значительных последствии.
Недоношенность Пределы жизнеспособности (limit of viability) – самый ранний гестационный возрат при котором шанс выживаемости не менее 50%. В развитых странах около 50% новорожденных при гестационном возрате 24 недели выживают. При этом половина из них инвалидизированна. 80% новорожденных, при гестационном возрате 28 недель, выживают без значительных последствии.
 Alveoli week 20 Alveoli week 24
Alveoli week 20 Alveoli week 24
 Anatomija Сурфактант синтезируется пнемоцитами type II на 24 -26 неделе гестации Заменная сурфактантная терапия (FDA -1990) значительно уменьшает смертность новорожденных от СДР, но не имеет очевидного влияния на частоту БЛД у новорожденных с эмвт.
Anatomija Сурфактант синтезируется пнемоцитами type II на 24 -26 неделе гестации Заменная сурфактантная терапия (FDA -1990) значительно уменьшает смертность новорожденных от СДР, но не имеет очевидного влияния на частоту БЛД у новорожденных с эмвт.
 Эффективность спонтанного дыхания
Эффективность спонтанного дыхания
 Эффективность спонтанного дыхания зависит от: Объёма газа Работы дыхания Резистентности дыхательных путей
Эффективность спонтанного дыхания зависит от: Объёма газа Работы дыхания Резистентности дыхательных путей
 Pulmonary mechanics Location of airway resistance: Resistance 0 5 Distal --> 10 15 20 Airway Generation В дистальной части дыхательной системы резистентность меньше из-за большой площади поперечного сечения ЭТТ маленького размера и скоростной поток могут значительно могут увеличить резистентность.
Pulmonary mechanics Location of airway resistance: Resistance 0 5 Distal --> 10 15 20 Airway Generation В дистальной части дыхательной системы резистентность меньше из-за большой площади поперечного сечения ЭТТ маленького размера и скоростной поток могут значительно могут увеличить резистентность.
 Pressure Port Flow from Ventilator Y – Piece to Tubus This is the Resistance „work of breathing“
Pressure Port Flow from Ventilator Y – Piece to Tubus This is the Resistance „work of breathing“
 При уменьшении диаметра трахеи в 2") Airway Resistance WOB - J/min Trachea diameter (mm) При уменьшении диаметра трахеи в 2 раза, работа дыхания (WOB) увеличивается в 16 раз!
Airway Resistance WOB - J/min Trachea diameter (mm) При уменьшении диаметра трахеи в 2 раза, работа дыхания (WOB) увеличивается в 16 раз!
 Airway Generation Development anatomy of respiratory tract Turbulent flow in Conductive area Air stream flow rate– 100 cm/s Laminar flow in: Transitory area Air stream flow rate – 1 cm/s Respiratory area Air stream flow rate – 0, 2 cm/s
Airway Generation Development anatomy of respiratory tract Turbulent flow in Conductive area Air stream flow rate– 100 cm/s Laminar flow in: Transitory area Air stream flow rate – 1 cm/s Respiratory area Air stream flow rate – 0, 2 cm/s
 Airway Resistance Newborn 20 -40 cm. H 2 O/L/sec ET 150 cm. H 2 O/L/sec) RDS >40 cm. H 2 O/L/sec BPD >150 cm. H 2 O/L/sec Adult 1 -2 cm. H 2 O/L/sec Tubus fixation – and where and how he get the needed tidal volume ? ? ? !!! Infants: nasal resistance 30 -50% of total NG tube increases total resistance up to 50%
Airway Resistance Newborn 20 -40 cm. H 2 O/L/sec ET 150 cm. H 2 O/L/sec) RDS >40 cm. H 2 O/L/sec BPD >150 cm. H 2 O/L/sec Adult 1 -2 cm. H 2 O/L/sec Tubus fixation – and where and how he get the needed tidal volume ? ? ? !!! Infants: nasal resistance 30 -50% of total NG tube increases total resistance up to 50%
 эндотрахеальная интубация 17 Even the basic procedure of endotracheal ventilation requires skills that are not trivial. Only 62% out of 60 attempts were successful in 31 infants during neonatal resuscitation (O'Donnell CP Pediatrics. 2006). Ø Success rates and mean+SD time to intubate: Residents: 24%, 49+13 sec; Fellows: 78%, 32+13 sec; Consultants: 86%, 25+17 sec. Infants frequently deteriorate during intubation attempts. Thus, to avoid these, NRS is required. Ø Ø
эндотрахеальная интубация 17 Even the basic procedure of endotracheal ventilation requires skills that are not trivial. Only 62% out of 60 attempts were successful in 31 infants during neonatal resuscitation (O'Donnell CP Pediatrics. 2006). Ø Success rates and mean+SD time to intubate: Residents: 24%, 49+13 sec; Fellows: 78%, 32+13 sec; Consultants: 86%, 25+17 sec. Infants frequently deteriorate during intubation attempts. Thus, to avoid these, NRS is required. Ø Ø
 Как помочь новорожденному дышать? Увеличить перфузию Улучить лёгочный compliance и стабилизировать грудную стенку (compliance is reduced: from 1 -2 to 0. 2 -0. 5 ml/cm. H 2 Okg) Уменьшить резистентность дых. путей Стратегическая идея – открыть лёгкие (recruitment of the lungs), и увеличить функциональную остаточную ёмкость (functional residual capacity-FRC reduction from 30 ml/kg, to as low as 4 -5 ml/kg. ), оберегая альвеолы от коллапса.
Как помочь новорожденному дышать? Увеличить перфузию Улучить лёгочный compliance и стабилизировать грудную стенку (compliance is reduced: from 1 -2 to 0. 2 -0. 5 ml/cm. H 2 Okg) Уменьшить резистентность дых. путей Стратегическая идея – открыть лёгкие (recruitment of the lungs), и увеличить функциональную остаточную ёмкость (functional residual capacity-FRC reduction from 30 ml/kg, to as low as 4 -5 ml/kg. ), оберегая альвеолы от коллапса.
 Как помочь новорожденному дышать, применяя респираторную аппаратуру? VENTILATION: Invasive via Endotracheal Tube: conventional, new modes - high frequency, pressure support, volume targeted, and synchronized ventilation Non-invasive: (Kugelman, 2010, Montreux) (S)NIPPV nasal intermittent positive pressure ventilation or (S)NIMV - nasal intermittent mandatory ventilation – назальная принудительная вентиляция, NCPAP - постоянное положительное давление в дыхательных путях (ППДДП), HFNC (high flow nasal cannula) – назальные канюли высокого потока (0. 5 -8 l/min. )
Как помочь новорожденному дышать, применяя респираторную аппаратуру? VENTILATION: Invasive via Endotracheal Tube: conventional, new modes - high frequency, pressure support, volume targeted, and synchronized ventilation Non-invasive: (Kugelman, 2010, Montreux) (S)NIPPV nasal intermittent positive pressure ventilation or (S)NIMV - nasal intermittent mandatory ventilation – назальная принудительная вентиляция, NCPAP - постоянное положительное давление в дыхательных путях (ППДДП), HFNC (high flow nasal cannula) – назальные канюли высокого потока (0. 5 -8 l/min. )
 History 1971 Gregory preterm RDS treatment through ET 20
History 1971 Gregory preterm RDS treatment through ET 20
 СДР – главная причина смертности и заболеваеемости недон. детей. Внедрение NCPAP – уменьшило смертность от этого заболевания около 2 раза. 21 June 1, 2011, Volume 127, Issue 6 Neonatal Mortality From Respiratory Distress Syndrome: Lessons for Low-Resource Countries Beena D. Kamath, MD, MPHa, Emily R. Mac. Guire, MSW, MPHb, Elizabeth M. Mc. Clure, MEdb, Robert L. Goldenberg, MDc, Alan H. Jobe, MD, Ph. Da ABSTRACT Respiratory distress syndrome (RDS) is a major contributor to neonatal mortality worldwide. However, little information is available regarding rates of RDS-specific mortality in low-income countries, and technologies for RDS treatment are used inconsistently in different health care settings. Our objective was to better understand the interventions that have decreased the rates of RDS-specific mortality in high-income countries over the past 60 years. We then estimated the effects on RDS-specific mortality in low-resource settings. Of the sequential introduction of technologies and therapies for RDS, widespread use of oxygen and continuous positive airway pressure were associated with the time periods that demonstrated the greatest decline in RDS-specific mortality. We argue that these 2 interventions applied widely in low-resource settings, with appropriate supportive infrastructure and general newborn care, will have the greatest impact on decreasing neonatal mortality. This historical perspective can inform policy-makers for the prioritization of scarce resources to improve survival rates for newborns worldwide. Accepted January 6, 2011. Copyright © 2011 by the American Academy of Pediatrics Neonatal Mortality From Respiratory Distress Syndrome: Lessons for Low-Resource Countries Page 2 of 2 http: //
СДР – главная причина смертности и заболеваеемости недон. детей. Внедрение NCPAP – уменьшило смертность от этого заболевания около 2 раза. 21 June 1, 2011, Volume 127, Issue 6 Neonatal Mortality From Respiratory Distress Syndrome: Lessons for Low-Resource Countries Beena D. Kamath, MD, MPHa, Emily R. Mac. Guire, MSW, MPHb, Elizabeth M. Mc. Clure, MEdb, Robert L. Goldenberg, MDc, Alan H. Jobe, MD, Ph. Da ABSTRACT Respiratory distress syndrome (RDS) is a major contributor to neonatal mortality worldwide. However, little information is available regarding rates of RDS-specific mortality in low-income countries, and technologies for RDS treatment are used inconsistently in different health care settings. Our objective was to better understand the interventions that have decreased the rates of RDS-specific mortality in high-income countries over the past 60 years. We then estimated the effects on RDS-specific mortality in low-resource settings. Of the sequential introduction of technologies and therapies for RDS, widespread use of oxygen and continuous positive airway pressure were associated with the time periods that demonstrated the greatest decline in RDS-specific mortality. We argue that these 2 interventions applied widely in low-resource settings, with appropriate supportive infrastructure and general newborn care, will have the greatest impact on decreasing neonatal mortality. This historical perspective can inform policy-makers for the prioritization of scarce resources to improve survival rates for newborns worldwide. Accepted January 6, 2011. Copyright © 2011 by the American Academy of Pediatrics Neonatal Mortality From Respiratory Distress Syndrome: Lessons for Low-Resource Countries Page 2 of 2 http: //
 Почему мы обсуждаем проблему инвазивной и неинвазивной вентиляции лёгких? 22 В Скандинавии уже многие годы начало лечения СДР методом NCPAP является рутинной практикой. Это почти 20 -летнее активное противостояние многим Западным странам (Англии, США), где предпочтение давалось - “более безопасной” принудительной ЭТ ИВЛ , особенно в конце 80 -ых, когда применение схемы - сурфактант + ЭТ ИВЛ= “золотой стандарт” лечения СДР
Почему мы обсуждаем проблему инвазивной и неинвазивной вентиляции лёгких? 22 В Скандинавии уже многие годы начало лечения СДР методом NCPAP является рутинной практикой. Это почти 20 -летнее активное противостояние многим Западным странам (Англии, США), где предпочтение давалось - “более безопасной” принудительной ЭТ ИВЛ , особенно в конце 80 -ых, когда применение схемы - сурфактант + ЭТ ИВЛ= “золотой стандарт” лечения СДР
 - 1998 Huddinge, Astrid Lindgrens Children’s Hospital, Stockholm, Sweden Оротрахеальная интубация Сурфактант") INSURE (Intubation/Surfactant/Extubation) - 1998 Huddinge, Astrid Lindgrens Children’s Hospital, Stockholm, Sweden Оротрахеальная интубация Сурфактант (100 мг/кг Куросурф); Экстубация СPAP.
INSURE (Intubation/Surfactant/Extubation) - 1998 Huddinge, Astrid Lindgrens Children’s Hospital, Stockholm, Sweden Оротрахеальная интубация Сурфактант (100 мг/кг Куросурф); Экстубация СPAP.
 Should we Administer Surfactant & Extubate Immediately to NCPAP? - “Scandinavian Model” NCPAP & prophylactic surfactant (vs. CMV and prophylactic surfactant): NCPAP-Surf decreased the number of infants ventilated at 7 days and the duration of O 2 therapy (Dani et al). NCPAP and prophylactic surfactant (and rapid extubation) vs. NCPAP (with later treatment if needed). Earlier use of CPAP+surfactant decreased the need for CMV (Verder & Reininger). Overall need for mechanical ventilation reduced by 50%
Should we Administer Surfactant & Extubate Immediately to NCPAP? - “Scandinavian Model” NCPAP & prophylactic surfactant (vs. CMV and prophylactic surfactant): NCPAP-Surf decreased the number of infants ventilated at 7 days and the duration of O 2 therapy (Dani et al). NCPAP and prophylactic surfactant (and rapid extubation) vs. NCPAP (with later treatment if needed). Earlier use of CPAP+surfactant decreased the need for CMV (Verder & Reininger). Overall need for mechanical ventilation reduced by 50%
 Не используя механ. принудительную ЭТ ИВЛ,") Фундаментальные концепции повреждении лёгких у новорожденных: (Polin, 2005) Не используя механ. принудительную ЭТ ИВЛ, сложно вызвать БЛД у новорожденного Даже кратковременное положительное давление при ИВЛ может инициировать воспалительный каскад, создавая условия для развития БЛД, особенно при дефиците сурфактанта. Главную роль в патогенезе БЛД играет повреждение, вызванное свободными радикалами.
Фундаментальные концепции повреждении лёгких у новорожденных: (Polin, 2005) Не используя механ. принудительную ЭТ ИВЛ, сложно вызвать БЛД у новорожденного Даже кратковременное положительное давление при ИВЛ может инициировать воспалительный каскад, создавая условия для развития БЛД, особенно при дефиците сурфактанта. Главную роль в патогенезе БЛД играет повреждение, вызванное свободными радикалами.
 являлась причиной значительных") Механическая эндотрахеальная вентиляция Даже коротковременная вентиляция (в эксперементе с недоношенными животными) являлась причиной значительных повреждении лёгких. Механическая вентиляция сама по себе является независимым фактором риска церебрального паралича и отставания развития недоношенных детей. (Ramanathan, Neonatology 2008; 93: 302 -308)
Механическая эндотрахеальная вентиляция Даже коротковременная вентиляция (в эксперементе с недоношенными животными) являлась причиной значительных повреждении лёгких. Механическая вентиляция сама по себе является независимым фактором риска церебрального паралича и отставания развития недоношенных детей. (Ramanathan, Neonatology 2008; 93: 302 -308)
 Эндотрахеальная ИВЛ Несмотря на новые методы ИВЛ (высокочастотная, двойнного контроля - давлением и объёмом, синхронизированная вентиляция) и применение сурфактанта , бронхолёгочная дисплазия – остаётся основной причиной заболеваемости у недоношенных детей, и её частота зависит от использования механической эт. ИВЛ. Так как нет доказательств о преимуществе какого-либо из аппаратов ИВЛ в уменьшении частоты БЛД, лучший подход – при возможности избегать эт. ИВЛ. *European consensus guidelines on the management of neonatal respiratory distress syndrome, J. Perinat. Med(2007)
Эндотрахеальная ИВЛ Несмотря на новые методы ИВЛ (высокочастотная, двойнного контроля - давлением и объёмом, синхронизированная вентиляция) и применение сурфактанта , бронхолёгочная дисплазия – остаётся основной причиной заболеваемости у недоношенных детей, и её частота зависит от использования механической эт. ИВЛ. Так как нет доказательств о преимуществе какого-либо из аппаратов ИВЛ в уменьшении частоты БЛД, лучший подход – при возможности избегать эт. ИВЛ. *European consensus guidelines on the management of neonatal respiratory distress syndrome, J. Perinat. Med(2007)
 БЛД При рождении лёгкие – неповрежденные, БЛД – как маркер повреждения лёгких новорожденных, в некоторых странах интерпретируется теперь, как ятрогения Этиология БЛД: воспалит. процесс, окси стресс, генет. факторы. Главный – механ. ИВЛ C. C. Roehr (Charite University Hospital, Berlin) K. Bohlin (Karolinska University Hospital, Stockholm) Breath, September 2011, Vol. 8, No 1 the incidence of BPD 42% (BW 25% (BW 11% (BW 501– 750 g), 751– 1000 g), 1001– 1250 g), 1251– 1500 g). Fanaroff AA, Am J Obstet Gynecol. 2007 28
БЛД При рождении лёгкие – неповрежденные, БЛД – как маркер повреждения лёгких новорожденных, в некоторых странах интерпретируется теперь, как ятрогения Этиология БЛД: воспалит. процесс, окси стресс, генет. факторы. Главный – механ. ИВЛ C. C. Roehr (Charite University Hospital, Berlin) K. Bohlin (Karolinska University Hospital, Stockholm) Breath, September 2011, Vol. 8, No 1 the incidence of BPD 42% (BW 25% (BW 11% (BW 501– 750 g), 751– 1000 g), 1001– 1250 g), 1251– 1500 g). Fanaroff AA, Am J Obstet Gynecol. 2007 28
 “Старая” “Новая” Нарушение развития дистальных") Формы БЛД - классическая Фибропролиферация и воспаление (1967, Northway) “Старая” “Новая” Нарушение развития дистальных частей лёгких (2001, Jobe, Bancalari)
Формы БЛД - классическая Фибропролиферация и воспаление (1967, Northway) “Старая” “Новая” Нарушение развития дистальных частей лёгких (2001, Jobe, Bancalari)
 Гестация <32 >32 Кислород >21% ≥ 28 d. Исходная") Критерии БЛД (2001 m. ) Гестация <32 >32 Кислород >21% ≥ 28 d. Исходная точка оценки 36 нед. гестации >28, <56 d. БЛД Лёгкая 21% O 2 36 нед. гестации Средняя <30% O 2 36 sav. гестации тяжёлая >30% O 2(ИВЛ или CPAP) 36 sav. Гест. 21% O 2 56 d. <30% O 2 56 d. >30% O 2(ИВЛ или CPAP) 56 d.
Критерии БЛД (2001 m. ) Гестация <32 >32 Кислород >21% ≥ 28 d. Исходная точка оценки 36 нед. гестации >28, <56 d. БЛД Лёгкая 21% O 2 36 нед. гестации Средняя <30% O 2 36 sav. гестации тяжёлая >30% O 2(ИВЛ или CPAP) 36 sav. Гест. 21% O 2 56 d. <30% O 2 56 d. >30% O 2(ИВЛ или CPAP) 56 d.
 при самостоятельном дыхании Основная цель НРП – использовать “мягкую”") Неинвазивная =назальная респираторная поддержка (НРП) при самостоятельном дыхании Основная цель НРП – использовать “мягкую” респираторную поддержку недоношенным новорожденным с СДР, избегая эндотрахеальную ИВЛ. НРП, как стартовый метод ИВЛ, уменьшает частоту БЛД. *European consensus guidelines on the management of neonatal respiratory distress syndrome, J. Perinat. Med(2007)
Неинвазивная =назальная респираторная поддержка (НРП) при самостоятельном дыхании Основная цель НРП – использовать “мягкую” респираторную поддержку недоношенным новорожденным с СДР, избегая эндотрахеальную ИВЛ. НРП, как стартовый метод ИВЛ, уменьшает частоту БЛД. *European consensus guidelines on the management of neonatal respiratory distress syndrome, J. Perinat. Med(2007)
 НРП в периферических ОРИТН 32 Для современной механической вентиляции необходим опытный персонала и дорогостоящая аппаратура. НРП и сурфактант снижает потребность в механической вентиляции. CPAP надёжен при транспортировке (Murray, Pediatrics 2008).
НРП в периферических ОРИТН 32 Для современной механической вентиляции необходим опытный персонала и дорогостоящая аппаратура. НРП и сурфактант снижает потребность в механической вентиляции. CPAP надёжен при транспортировке (Murray, Pediatrics 2008).
 Как действует CPAP? Увеличивает транспульмональное давление → предотвращает коллапс альвеол → увеличивает остаточную емкость легких (FRC); → увеличивается объём поверхности для газообмена → уменьшает сопротивляемость в дыхательных путях → улучшаеться синтез эндогенного сурфактанта → уменьшает потребность в кислороде → уменьшает риск токсического воздействия O 2 Соответсвенно улучшает соотношение вентиляция/перфузия; стабилизирует ритм дыхания и минутную вентиляцию; улучшает эластичность и compliance лёгких; уменьшает работу дыхания; По сравнению с ЭТ ИВЛ, CPAP: способствует нормальному мукоцилиарному транспорту в дых. путях, меньшая возможность баротравмы легких, меньше риск вторичной инфекции
Как действует CPAP? Увеличивает транспульмональное давление → предотвращает коллапс альвеол → увеличивает остаточную емкость легких (FRC); → увеличивается объём поверхности для газообмена → уменьшает сопротивляемость в дыхательных путях → улучшаеться синтез эндогенного сурфактанта → уменьшает потребность в кислороде → уменьшает риск токсического воздействия O 2 Соответсвенно улучшает соотношение вентиляция/перфузия; стабилизирует ритм дыхания и минутную вентиляцию; улучшает эластичность и compliance лёгких; уменьшает работу дыхания; По сравнению с ЭТ ИВЛ, CPAP: способствует нормальному мукоцилиарному транспорту в дых. путях, меньшая возможность баротравмы легких, меньше риск вторичной инфекции
 Indications for NRS - начальное лечение СДР, ранний период после экстубации профилактический CPAP для детей с очень низкой массой тела – в родзале апноэ новорожденных транзиторная тахипнея National Guideline Clearinghouse 2008/03/11 Respiratory insuff. , resp. rate 30% more than normal Blood gases – delivering Fi. O 2 60%, Pa. O 2 less than 50 torr, PCO 2 > 50 torr, p. H – 7. 25 Abnormal chest X-ray
Indications for NRS - начальное лечение СДР, ранний период после экстубации профилактический CPAP для детей с очень низкой массой тела – в родзале апноэ новорожденных транзиторная тахипнея National Guideline Clearinghouse 2008/03/11 Respiratory insuff. , resp. rate 30% more than normal Blood gases – delivering Fi. O 2 60%, Pa. O 2 less than 50 torr, PCO 2 > 50 torr, p. H – 7. 25 Abnormal chest X-ray
 Давление NCPAP Мета-анализы исследовании доказывают, что как правило, адекватно давление NCPAP 5 -6 cm H 2 O. What pressure range should be used? No randomised trials have been identified on this question. Conventionally, a nasal CPAP of 5 cm H 2 O is used, rising in 1 cm increments to 10 cm. if there is no improvement. Higher levels may over-distend the lungs, leading to hypercapnia (De Paoli, 2002; Carlo, 2001). Carlo WA. Assisted ventilation. In: Klaus MH, Fanaroff AA (eds). Care of the high-risk neonate, 5 th ed. Philadelphia, W. B. Saunders, 2001. p. 283 De Paoli AG, Davis PG, Faber B, et al. Devices and pressure sources for administration of nasal continuous positive airway pressure (NCPAP) in preterm neonates. The Cochrane Database of Systematic Reviews 2002, Issue 3. Art. No. : CD 002977 Evidence Level: V Используя давление выше 8 cm H 2 O, повышается риск пневмоторакса (Morley CJ, N Engl J Med. 2008).
Давление NCPAP Мета-анализы исследовании доказывают, что как правило, адекватно давление NCPAP 5 -6 cm H 2 O. What pressure range should be used? No randomised trials have been identified on this question. Conventionally, a nasal CPAP of 5 cm H 2 O is used, rising in 1 cm increments to 10 cm. if there is no improvement. Higher levels may over-distend the lungs, leading to hypercapnia (De Paoli, 2002; Carlo, 2001). Carlo WA. Assisted ventilation. In: Klaus MH, Fanaroff AA (eds). Care of the high-risk neonate, 5 th ed. Philadelphia, W. B. Saunders, 2001. p. 283 De Paoli AG, Davis PG, Faber B, et al. Devices and pressure sources for administration of nasal continuous positive airway pressure (NCPAP) in preterm neonates. The Cochrane Database of Systematic Reviews 2002, Issue 3. Art. No. : CD 002977 Evidence Level: V Используя давление выше 8 cm H 2 O, повышается риск пневмоторакса (Morley CJ, N Engl J Med. 2008).
 Отлучение доказано преимущество метода отлучения постепенно уменьшая давление CPAP перед методом прерывания и возобновления CPAP терапии, что может быть связано с развитием БЛД (Singh S, Abstract, Europediatrics, Barcelona, October 2006). Критерии отлучения При Fi. O 2 <30% , исчезновение признаков дыхательного дистресса, нормальные газы крови. (Kugelman A, J Pediatr. 2007). How should infants be weaned from CPAP? “The optimal method of weaning infants from NCPAP remains unanswered” (Bowe, 2005). A postal survey of all 58 neonatal units with intensive care cots in the Northern Region (Bowe, 2005) found that 36 (66%) weaned on an ad-hoc basis by gradually decreasing pressure and that 16 (30%) had no set method. Only 3 units (6%) had a weaning protocol, although most (85%) felt that formal guidelines would be helpful. Bowe L, Clarke P. Current use of nasal continuous positive airways pressure in neonates. Arch Dis Child Fetal Neonatal Ed 2005; 90: F 92 -4 Evidence Level: V
Отлучение доказано преимущество метода отлучения постепенно уменьшая давление CPAP перед методом прерывания и возобновления CPAP терапии, что может быть связано с развитием БЛД (Singh S, Abstract, Europediatrics, Barcelona, October 2006). Критерии отлучения При Fi. O 2 <30% , исчезновение признаков дыхательного дистресса, нормальные газы крови. (Kugelman A, J Pediatr. 2007). How should infants be weaned from CPAP? “The optimal method of weaning infants from NCPAP remains unanswered” (Bowe, 2005). A postal survey of all 58 neonatal units with intensive care cots in the Northern Region (Bowe, 2005) found that 36 (66%) weaned on an ad-hoc basis by gradually decreasing pressure and that 16 (30%) had no set method. Only 3 units (6%) had a weaning protocol, although most (85%) felt that formal guidelines would be helpful. Bowe L, Clarke P. Current use of nasal continuous positive airways pressure in neonates. Arch Dis Child Fetal Neonatal Ed 2005; 90: F 92 -4 Evidence Level: V
![Критерии неудачной NCPAP терапии Клиническое ухудшение [прогрессирующий СДР], сопровождающееся ухудшением одного из показателей: 1.](https://present5.com/presentation/58489028_418926232/image-39.jpg "Критерии неудачной NCPAP терапии Клиническое ухудшение [прогрессирующий СДР], сопровождающееся ухудшением одного из показателей: 1.") Критерии неудачной NCPAP терапии Клиническое ухудшение [прогрессирующий СДР], сопровождающееся ухудшением одного из показателей: 1. p. H<7. 20 и PCO 2>60 mm. Hg, 2. Pa. O 2<50 mm. Hg или (Sp. O 2) <88% при Fi. O 2>50%, 3. Повторяющиеся апное, вынуждающие прибегать к использованию стимуляции механической вентиляцией мешком Амбу через маску, несмотря на применение метилксантинов. Во избежании эндотрахеальной интубации, с NCPAP возможно переключится на назальную перемежающуюся принудительную вентиляцию (Kugelman A. J Pediatr. 2007)
Критерии неудачной NCPAP терапии Клиническое ухудшение [прогрессирующий СДР], сопровождающееся ухудшением одного из показателей: 1. p. H<7. 20 и PCO 2>60 mm. Hg, 2. Pa. O 2<50 mm. Hg или (Sp. O 2) <88% при Fi. O 2>50%, 3. Повторяющиеся апное, вынуждающие прибегать к использованию стимуляции механической вентиляцией мешком Амбу через маску, несмотря на применение метилксантинов. Во избежании эндотрахеальной интубации, с NCPAP возможно переключится на назальную перемежающуюся принудительную вентиляцию (Kugelman A. J Pediatr. 2007)
 Противопоказания : диафрагмальная грыжа, атрезия хоан, расщелина мягкого и твёрдого нёба, трахеопищеводный свищь ОСЛОЖНЕНИЯ ТЕРАПИИ CPAP: - Закупорка или смещение назальных канюль или назофарингеальной трубки; - Перерастяжение желудка накапливающимся воздухом, затруднения вскармливания, срыгивание (аспирация пищей); - Пролежни, деформации, некроз носовой перегородки; --------------------------------------------------- Перерастяжение легких - пневмоторакс и/или интерстициальная эмфизема легких; - pa. CO 2 и работы дыхания (если CPAP>10 см Н 2 О ст. ); - Нарушение сердечного возврата крови и минутного объема (если CPAP>10 см Н 2 О ст. ); 40
Противопоказания : диафрагмальная грыжа, атрезия хоан, расщелина мягкого и твёрдого нёба, трахеопищеводный свищь ОСЛОЖНЕНИЯ ТЕРАПИИ CPAP: - Закупорка или смещение назальных канюль или назофарингеальной трубки; - Перерастяжение желудка накапливающимся воздухом, затруднения вскармливания, срыгивание (аспирация пищей); - Пролежни, деформации, некроз носовой перегородки; --------------------------------------------------- Перерастяжение легких - пневмоторакс и/или интерстициальная эмфизема легких; - pa. CO 2 и работы дыхания (если CPAP>10 см Н 2 О ст. ); - Нарушение сердечного возврата крови и минутного объема (если CPAP>10 см Н 2 О ст. ); 40
 infants born at") NRS/IRS - BPD Ø Ø Morley (N Engl J Med. 2008) infants born at 25 -to-28 -weeks' gestation, В гестационном возрасте 36 нед. В группе с CPAP терапией 33. 9% новорожденных умерли им установлен дгн. БЛД, по сравнению с 38. 9% соответствующих состоянии из интубированной группы (table 2) В возрасте 28 дней меньший показатель смертности и потребности в кислородном лечении в группе с CPAP терапией по сравнению с группой, в которой применялась интубация с ИВЛ (table 3)
NRS/IRS - BPD Ø Ø Morley (N Engl J Med. 2008) infants born at 25 -to-28 -weeks' gestation, В гестационном возрасте 36 нед. В группе с CPAP терапией 33. 9% новорожденных умерли им установлен дгн. БЛД, по сравнению с 38. 9% соответствующих состоянии из интубированной группы (table 2) В возрасте 28 дней меньший показатель смертности и потребности в кислородном лечении в группе с CPAP терапией по сравнению с группой, в которой применялась интубация с ИВЛ (table 3)
 42") ENCPAP&BPD - Trends in VLBW infants (Pediatrics 2005 , Aly H) 42
ENCPAP&BPD - Trends in VLBW infants (Pediatrics 2005 , Aly H) 42
 Data from a comparison of treatment of premature infants at the University of Vienna tertiary centre and the Vermont Oxford Neonatal Network as a whole (Kirchner, 2005) CPAP used Retinopathy BPD 45 -86% vs 1 -10% vs 14 -32% vs 37 -63% 8 -12% 27 -39%
Data from a comparison of treatment of premature infants at the University of Vienna tertiary centre and the Vermont Oxford Neonatal Network as a whole (Kirchner, 2005) CPAP used Retinopathy BPD 45 -86% vs 1 -10% vs 14 -32% vs 37 -63% 8 -12% 27 -39%
 Different treatment strategies of LWI in Columbian and Boston Universities NICU 1991 – 1993 Early CPAP ALV Surf. CLD Columbian NICU 63% 29% 10% Boston NICU 11% 75% 45% 22% 4% Van Marter. L. J. et al. Pediatrics 2000; 105(6): 1194 -201 44
Different treatment strategies of LWI in Columbian and Boston Universities NICU 1991 – 1993 Early CPAP ALV Surf. CLD Columbian NICU 63% 29% 10% Boston NICU 11% 75% 45% 22% 4% Van Marter. L. J. et al. Pediatrics 2000; 105(6): 1194 -201 44
 Resp. support, gest. age < 28 weeks 45 ALV day 1 ALV day 7 ALV day 28 Acta Paediatrica, 2007
Resp. support, gest. age < 28 weeks 45 ALV day 1 ALV day 7 ALV day 28 Acta Paediatrica, 2007
 Новое в неинвазивной вентиляции лёгких у новорожденных // © Vladimiras Chijenas, MD, 2011 47
Новое в неинвазивной вентиляции лёгких у новорожденных // © Vladimiras Chijenas, MD, 2011 47
 Новое в неинвазивной вентиляции лёгких у новорожденных // © Vladimiras Chijenas, MD, 2011 48
Новое в неинвазивной вентиляции лёгких у новорожденных // © Vladimiras Chijenas, MD, 2011 48
 Использование сурфактанта SURFAKTANTO PANAUDOJIMAS <32 sav. Kauno MUK NRITS 2003 2004 2005 2006 2007 2008 2009 2010 80 75 55 56 53 48 56 59 46(36. 5%) 41(35. 9%) 62(53%) 67(54. 5%) 61(53. 5%) 81(62. 8%) 66(54. 1%) 45(43. 3%) Dvi dozės 20 19 8 17 7 9 9 1 Trys dozės 3 1 - - - Viso dozių 69 61 70 84 68 90 75 42 Neskirta Skirta
Использование сурфактанта SURFAKTANTO PANAUDOJIMAS <32 sav. Kauno MUK NRITS 2003 2004 2005 2006 2007 2008 2009 2010 80 75 55 56 53 48 56 59 46(36. 5%) 41(35. 9%) 62(53%) 67(54. 5%) 61(53. 5%) 81(62. 8%) 66(54. 1%) 45(43. 3%) Dvi dozės 20 19 8 17 7 9 9 1 Trys dozės 3 1 - - - Viso dozių 69 61 70 84 68 90 75 42 Neskirta Skirta
 gestacija iki") Антенатальная профилактика созревания лёгких кортикостеройдами PLAUČIŲ BRANDINIMAS – DPV ( deksametazonas, β-metazonas) gestacija iki 30 sav. Kauno MUK NRITS 2003 DPV po brandinimo ИВЛ -при антенат. кортикостеройдах DPV nebrandintiems ИВЛ - без антенат. кортикостеройдов 2004 2005 2006 2007 2008 2009 2010 58 45 39 54 45 (51. 9%) 34 38 (67. 4%) (78. 9%) (78. 9% (60%) (65. 1%) (65. 1% 52 46. 5%) 46 44. 7%) (41. 5%) 30 40 36 30 20 20 33 18 (78. 9%) (75. 5%) (75%) (78. 9%) (62. 5% (71. 4%) (71. 7%) (75%)
Антенатальная профилактика созревания лёгких кортикостеройдами PLAUČIŲ BRANDINIMAS – DPV ( deksametazonas, β-metazonas) gestacija iki 30 sav. Kauno MUK NRITS 2003 DPV po brandinimo ИВЛ -при антенат. кортикостеройдах DPV nebrandintiems ИВЛ - без антенат. кортикостеройдов 2004 2005 2006 2007 2008 2009 2010 58 45 39 54 45 (51. 9%) 34 38 (67. 4%) (78. 9%) (78. 9% (60%) (65. 1%) (65. 1% 52 46. 5%) 46 44. 7%) (41. 5%) 30 40 36 30 20 20 33 18 (78. 9%) (75. 5%) (75%) (78. 9%) (62. 5% (71. 4%) (71. 7%) (75%)
 51 Заболеваемость БЛД и выживаемость у детей 500 – 1500 г. (КМУ, клиника неонатологии, ОРИТН) Новое в неинвазивной вентиляции лёгких у новорожденных // © Vladimiras Chijenas, MD, 2011
51 Заболеваемость БЛД и выживаемость у детей 500 – 1500 г. (КМУ, клиника неонатологии, ОРИТН) Новое в неинвазивной вентиляции лёгких у новорожденных // © Vladimiras Chijenas, MD, 2011
 Neonatology 2010; 97: 402– 417 DOI: 10. 1159/000297773 52 European Consensus Guidelines on the Management of Neonatal Respiratory Distress Syndrome in Preterm Infants – 2010 Update David G. Sweet, Virgilio Carnielli, Gorm Greisen, Mikko Hallman, Eren Ozek, Richard Plavka, Ola D. Saugstad, Umberto Simeoni, Christian P. Speer, Henry L. Halliday These updated guidelines contain new evidence from recent Cochrane reviews and the medical literature since 2007. Many of the previous recommendations regarding early surfactant and CPAP are now more firmly evidence-based. The section on delivery room stabilisation has been considerably expanded. There are new recommendations on delaying umbilical cord clamping and a new section has been added on avoiding or reducing duration of mechanical ventilation, including recommendations on caffeine therapy, nasal ventilation, permissive hypercapnia and the role of newer ventilator modalities. A new ‘miscellaneous’ section has also been added covering aspects of RDS management that arise infrequently. Ранний сурфактант и CPAP, назальная ИВЛ, пермиссивная гиперкапния, избегать или укорачивать время применения ИВЛ, замедление пережатия пуповины, лечение кофеином и др.
Neonatology 2010; 97: 402– 417 DOI: 10. 1159/000297773 52 European Consensus Guidelines on the Management of Neonatal Respiratory Distress Syndrome in Preterm Infants – 2010 Update David G. Sweet, Virgilio Carnielli, Gorm Greisen, Mikko Hallman, Eren Ozek, Richard Plavka, Ola D. Saugstad, Umberto Simeoni, Christian P. Speer, Henry L. Halliday These updated guidelines contain new evidence from recent Cochrane reviews and the medical literature since 2007. Many of the previous recommendations regarding early surfactant and CPAP are now more firmly evidence-based. The section on delivery room stabilisation has been considerably expanded. There are new recommendations on delaying umbilical cord clamping and a new section has been added on avoiding or reducing duration of mechanical ventilation, including recommendations on caffeine therapy, nasal ventilation, permissive hypercapnia and the role of newer ventilator modalities. A new ‘miscellaneous’ section has also been added covering aspects of RDS management that arise infrequently. Ранний сурфактант и CPAP, назальная ИВЛ, пермиссивная гиперкапния, избегать или укорачивать время применения ИВЛ, замедление пережатия пуповины, лечение кофеином и др.
 – один") Acronym Definition Nasal N CPAP NCPAP-терапия (Nasal Continous Positive Airway ( Pressure) – один из методов неинвазивной ИВЛ (Wiswell & Srinivasan, 2003). Это метод лечение пациента, находящегося на самостоятельном дыхании, позволяет создать и поддерживать постоянное положительное давление в дыхательных путях (ППДДП), тем самым обеспечивая их проходимость и препядствуя коллапсу алвеол. intra alveoli pressure cm H 2 O Continous Positive Airway Pressure 6 5 E 4 3 постоянное положительное давление в дыхательных путях (ППДДП) E I I 2 1 Zeitachse
Acronym Definition Nasal N CPAP NCPAP-терапия (Nasal Continous Positive Airway ( Pressure) – один из методов неинвазивной ИВЛ (Wiswell & Srinivasan, 2003). Это метод лечение пациента, находящегося на самостоятельном дыхании, позволяет создать и поддерживать постоянное положительное давление в дыхательных путях (ППДДП), тем самым обеспечивая их проходимость и препядствуя коллапсу алвеол. intra alveoli pressure cm H 2 O Continous Positive Airway Pressure 6 5 E 4 3 постоянное положительное давление в дыхательных путях (ППДДП) E I I 2 1 Zeitachse
 1940 high altitude flying 1967 adult") HISTORY 1930 Poulton & Oxon (via face mask) 1940 high altitude flying 1967 adult RDS treatment
HISTORY 1930 Poulton & Oxon (via face mask) 1940 high altitude flying 1967 adult RDS treatment
 55
55
 56 1973 год – первая статья об использовании назального СРАР – Jens Camper et al. • Fleming, Fanaroff, Klaus, et al. Pediatrics 1973; 52: 131 A Device for Administration of CPAP by the Nasal Route • Caliumi-Pellegrini G, Agostino R, Orzalesi M, Nodari S, Marzetti G, Savignoni PG, et al. Arch Dis Child 1974; 49: 228– 30. Twin nasal cannula for administration of continuous positive airway pressure to newborn infants
56 1973 год – первая статья об использовании назального СРАР – Jens Camper et al. • Fleming, Fanaroff, Klaus, et al. Pediatrics 1973; 52: 131 A Device for Administration of CPAP by the Nasal Route • Caliumi-Pellegrini G, Agostino R, Orzalesi M, Nodari S, Marzetti G, Savignoni PG, et al. Arch Dis Child 1974; 49: 228– 30. Twin nasal cannula for administration of continuous positive airway pressure to newborn infants
 History 1970 - 1980 “Bubble” CPAP: Просто, но эффективно 57 © M. Kaneta
History 1970 - 1980 “Bubble” CPAP: Просто, но эффективно 57 © M. Kaneta
 F & P „ Bubble CPAP Prong - Adapter Gasblender for O 2/Air Tubing and Fixation F&P Humidifier 850 Prongs Adjustable waterlock for CPAP setting Bonnets Belts
F & P „ Bubble CPAP Prong - Adapter Gasblender for O 2/Air Tubing and Fixation F&P Humidifier 850 Prongs Adjustable waterlock for CPAP setting Bonnets Belts
 Dräger „Baby. Flow“ only with Babylog 8000 – passive n. CPAP
Dräger „Baby. Flow“ only with Babylog 8000 – passive n. CPAP
 HUDSON - CPAP Pressure measurement point Nasal Canulla Inspiration Expiration
HUDSON - CPAP Pressure measurement point Nasal Canulla Inspiration Expiration
 History 61 1968 Benveniste, Pedersen Принцип работы - “Физический Клапан Benveniste” – газ – инжекционная система, (gas-jet valve – Venturi principle creates continuous pressure ), described in neonatal practice in 1976
History 61 1968 Benveniste, Pedersen Принцип работы - “Физический Клапан Benveniste” – газ – инжекционная система, (gas-jet valve – Venturi principle creates continuous pressure ), described in neonatal practice in 1976
 CPAP measure 62 Patient Drive Flow History 1992 Moa et al. Переменный поток – INFANT FLOW - variable flow, Coanda effect Infant Flow n. CPAP generator, first introduction was 1992 in the UK, needs special flowdriver Expiration in- and outlet - jet
CPAP measure 62 Patient Drive Flow History 1992 Moa et al. Переменный поток – INFANT FLOW - variable flow, Coanda effect Infant Flow n. CPAP generator, first introduction was 1992 in the UK, needs special flowdriver Expiration in- and outlet - jet
 63 eme Infant Flow DB 350
63 eme Infant Flow DB 350
 Infant Flow Driver MK II & F&P Humidifier Si. PAP Biphasic is a timed bilevel pressure rise above baseline CPAP. Biphasic tr* Biphasic tr is a noninvasive synchronized nasal intermittent positive pressure ventilatory (SNIPPV) support modality that allows clinicians to provide respiratory support without the need for an endotracheal tube. *Not available in the United States
Infant Flow Driver MK II & F&P Humidifier Si. PAP Biphasic is a timed bilevel pressure rise above baseline CPAP. Biphasic tr* Biphasic tr is a noninvasive synchronized nasal intermittent positive pressure ventilatory (SNIPPV) support modality that allows clinicians to provide respiratory support without the need for an endotracheal tube. *Not available in the United States

 München with the Alps
München with the Alps
 Head office in Puchheim - München
Head office in Puchheim - München
 The Golden n. CPAP Generator – Benveniste valve 69 First Prototype 1996
The Golden n. CPAP Generator – Benveniste valve 69 First Prototype 1996
 70
70
 71 Manual Pushing activity Accessory kit for standard sindi SMPV S M P V synchron manual pressure ventilation Simply manual push activity to stimulate spontanious breathing and overcome apnoe
71 Manual Pushing activity Accessory kit for standard sindi SMPV S M P V synchron manual pressure ventilation Simply manual push activity to stimulate spontanious breathing and overcome apnoe
 Classification of NCPAP Henrik Verder, Kajsa Bohlin, Jens Kamper, Robert Lindwall, Baldvin Jonsson Acta Paediatrica, Volume 98, Issue 9, pages 1400– 1408, September 2009 Active systems (variable flow) - Переменный поток – CPAP создется специальным генератором, в котором разделяется инспираторный (поток подоваемой воздушно-кислородной смеси) и экспираторный поток. GENERATORS : Infant flow (Coanda effect) Medijet (Jet Injectors/Physical valve) Passive systems (continous flow) - Постоянный поток - система с клапаном выдоха - сосуд с налитой водой, - специальный механический клапан выдоха аппаратов ИВЛ 72
Classification of NCPAP Henrik Verder, Kajsa Bohlin, Jens Kamper, Robert Lindwall, Baldvin Jonsson Acta Paediatrica, Volume 98, Issue 9, pages 1400– 1408, September 2009 Active systems (variable flow) - Переменный поток – CPAP создется специальным генератором, в котором разделяется инспираторный (поток подоваемой воздушно-кислородной смеси) и экспираторный поток. GENERATORS : Infant flow (Coanda effect) Medijet (Jet Injectors/Physical valve) Passive systems (continous flow) - Постоянный поток - система с клапаном выдоха - сосуд с налитой водой, - специальный механический клапан выдоха аппаратов ИВЛ 72
 Is All NCPAP Created Equal? 73 Controlled clinical trials: Physiologic data • Courtney, Habib et al: Lung recruitment and breathing pattern during variable vs continuous flow NCPAP in premature infants: An evaluation of three devices. Pediatrics 2001 • Pandit, Courtney, Habib et al: Work of breathing during constant and variable flow NCPAP in preterm neonates. Pediatrics 2001 • Courtney, Habib et al: Changes in lung volume and work of breathing: A comparison of two variable flow NCPAP devices in VLBW infants. Pediatric Pulmonology 2003 Bottom Line: WOB less, lung recruitment better with variableflow.
Is All NCPAP Created Equal? 73 Controlled clinical trials: Physiologic data • Courtney, Habib et al: Lung recruitment and breathing pattern during variable vs continuous flow NCPAP in premature infants: An evaluation of three devices. Pediatrics 2001 • Pandit, Courtney, Habib et al: Work of breathing during constant and variable flow NCPAP in preterm neonates. Pediatrics 2001 • Courtney, Habib et al: Changes in lung volume and work of breathing: A comparison of two variable flow NCPAP devices in VLBW infants. Pediatric Pulmonology 2003 Bottom Line: WOB less, lung recruitment better with variableflow.
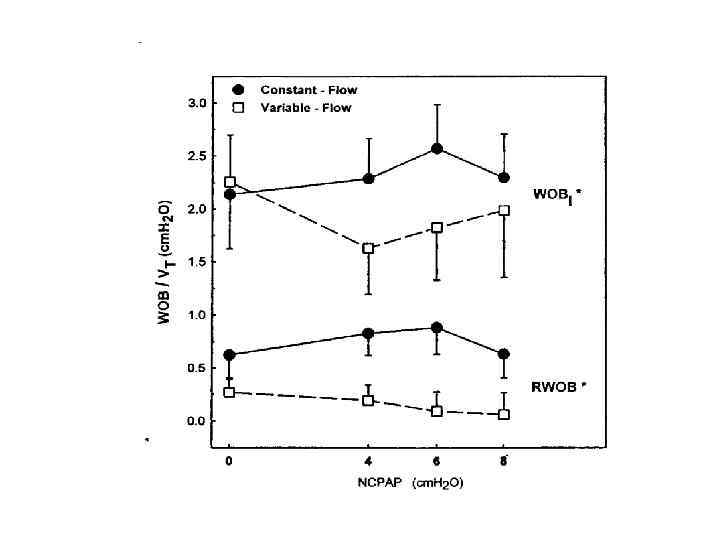
 Boumecid H, Rakza T, Abazine A, et al. Influence of three nasal continuous positive airway pressure devices on breathing pattern in preterm infants. Arch Dis Child Fetal Neonatal Ed 2007; 92: F 298 -300 A small study in 13 premature infants (Boumecid, 2007) suggests that variable-flow NCPAP increases tidal volume and improves thoraco-abdominal synchrony to a greater extent than is the case with constant-flow NCPAP and nasal prongs. Доказано преимущество в применении variable-flow NCPAP над constant-flow NCPAP с использованием назальных канюль: в увеличении минутного объёма дыхания улучшении торако-абдоминальной синхронизации и
Boumecid H, Rakza T, Abazine A, et al. Influence of three nasal continuous positive airway pressure devices on breathing pattern in preterm infants. Arch Dis Child Fetal Neonatal Ed 2007; 92: F 298 -300 A small study in 13 premature infants (Boumecid, 2007) suggests that variable-flow NCPAP increases tidal volume and improves thoraco-abdominal synchrony to a greater extent than is the case with constant-flow NCPAP and nasal prongs. Доказано преимущество в применении variable-flow NCPAP над constant-flow NCPAP с использованием назальных канюль: в увеличении минутного объёма дыхания улучшении торако-абдоминальной синхронизации и
 Flow and Pressure relation with passive n. CPAP devices
Flow and Pressure relation with passive n. CPAP devices
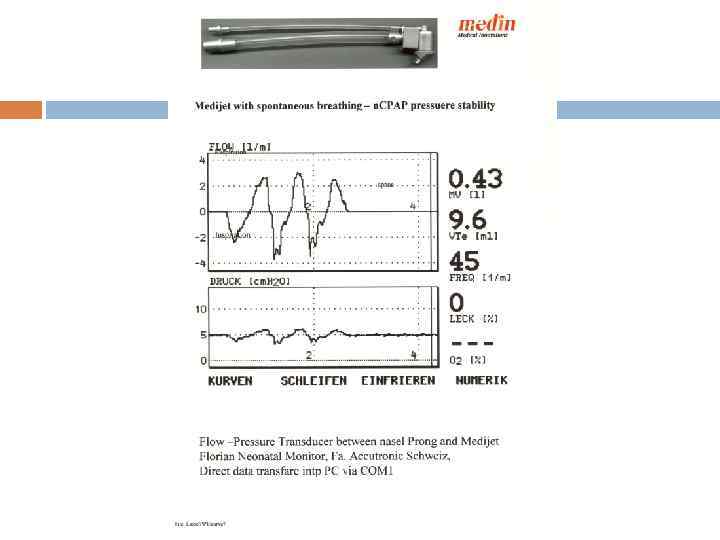
 CPAP measure 78 Patient Drive Flow Expiration in- and outlet - jet
CPAP measure 78 Patient Drive Flow Expiration in- and outlet - jet
 79
79
. 2003 Apr; 58(4): 350 -6. [Nasal continuous positive") IF vs Medijet An Pediatr (Barc). 2003 Apr; 58(4): 350 -6. [Nasal continuous positive airway pressure in preterm infants: comparison of two low-resistance models]. [Article in Spanish] Gutiérrez Laso A, Sáenz González P, Izquierdo Macián I, Fernández Gilino C, Gimeno Navarro A, Gormaz Moreno M, Torres Palomares D, Morcillo Sopena F, Roqués Serradilla V. Unidad de Cuidados Intensivos. Servicio de Neonatología. Hospital Universitario La Fe. Valencia. España. aguti@teleline. es Abstract OBJECTIVE: To compare the safety and efficacy of two low expiratory resistance models of nasal continuous positive airway pressure (n-CPAP) in preterm infants. MATERIAL AND METHODS: A 1 -year prospective trial was performed in the Neonatal Intensive Care Unit of La Fe Hospital to compare the Infant Flow (IF) and Medijet (MJ) devices. All preterm infants requiring n-CPAP for respiratory distress at birth (group I), infants weighting less than 1500 g requiring postextubation (group II) and those with apneabradycardia syndrome (ABS) (group III) were included. The patients were randomly assigned to IF or MJ. RESULTS: A total of 125 patients received 226 treatments (IF: n 5 126: MJ: n 5 110). The mean gestational age was 29. 4 weeks and the mean birth weight was 1340 g. Efficacy. In group I (n 5 73) no difference were found between systems and 6 hours' after initiation of n-CPAP decreases in Fi. O 2, CO 2 and respiratory effort were similar. The need for intubation was also similar (IF: 34. 6 %; MJ: 24. 1 %). In group II (n 5 73) the need for reintubation at 48 hours was similar with both treatments (IF: 19 %; MJ: 8 %). In group III (n 5 80) resolution of ABS was similar after 24 hours of n-CPAP (IF: 46 %; MJ: 58 %). The need for intubation was also similar (IF: 26 %; MJ: 10 %). Complications. Air leaks occurred in six preterm infants (IF: 4; MJ: 2). Severe abdominal distension occurred in 5 % with both systems. Five infants had significant nasal lesions (IF: 1; MJ: 4). CONCLUSIONS: The efficacy and safety of both systems was similar in the variables studied and no significant 80 differences were found.
IF vs Medijet An Pediatr (Barc). 2003 Apr; 58(4): 350 -6. [Nasal continuous positive airway pressure in preterm infants: comparison of two low-resistance models]. [Article in Spanish] Gutiérrez Laso A, Sáenz González P, Izquierdo Macián I, Fernández Gilino C, Gimeno Navarro A, Gormaz Moreno M, Torres Palomares D, Morcillo Sopena F, Roqués Serradilla V. Unidad de Cuidados Intensivos. Servicio de Neonatología. Hospital Universitario La Fe. Valencia. España. aguti@teleline. es Abstract OBJECTIVE: To compare the safety and efficacy of two low expiratory resistance models of nasal continuous positive airway pressure (n-CPAP) in preterm infants. MATERIAL AND METHODS: A 1 -year prospective trial was performed in the Neonatal Intensive Care Unit of La Fe Hospital to compare the Infant Flow (IF) and Medijet (MJ) devices. All preterm infants requiring n-CPAP for respiratory distress at birth (group I), infants weighting less than 1500 g requiring postextubation (group II) and those with apneabradycardia syndrome (ABS) (group III) were included. The patients were randomly assigned to IF or MJ. RESULTS: A total of 125 patients received 226 treatments (IF: n 5 126: MJ: n 5 110). The mean gestational age was 29. 4 weeks and the mean birth weight was 1340 g. Efficacy. In group I (n 5 73) no difference were found between systems and 6 hours' after initiation of n-CPAP decreases in Fi. O 2, CO 2 and respiratory effort were similar. The need for intubation was also similar (IF: 34. 6 %; MJ: 24. 1 %). In group II (n 5 73) the need for reintubation at 48 hours was similar with both treatments (IF: 19 %; MJ: 8 %). In group III (n 5 80) resolution of ABS was similar after 24 hours of n-CPAP (IF: 46 %; MJ: 58 %). The need for intubation was also similar (IF: 26 %; MJ: 10 %). Complications. Air leaks occurred in six preterm infants (IF: 4; MJ: 2). Severe abdominal distension occurred in 5 % with both systems. Five infants had significant nasal lesions (IF: 1; MJ: 4). CONCLUSIONS: The efficacy and safety of both systems was similar in the variables studied and no significant 80 differences were found.
 Summary Report on n. CPAP devices Technical Highschool Furtwangen - Germany Prof. Dr. Ing. Bernhard Vondenbusch Steinbeis Transfercentre Biomedical Engineering, 2007 In the present report the major characteristics of n. CPAP generators were investigated and compared to each other -high feeding pressure(85 cm. H 2 O) Высокое поддерживащие давление -high noise (74 -79/102 db. A) Сильный шум -aggresive insp. Flow (jet is directly running into the nostrils ) Аггресивный поток смеси в ноздри Infant Flow – fluidic flip technic (Coanda effect) -low feeding pressure (10 cm. H 2 O) -low noise (62 -68 db. A) -volume reservoir (jet is indirectly running at 90° ) Medijet – all types – Benveniste valve +: Range of prongs (3 vs 6) and masks(1 vs 3) -Bonnets with open back for neurosonography and infusions -Generators (1 disposable vs 1 disposable with changing angle and drug nebulizing port and 2 types of reusable), flexible fixation 81
Summary Report on n. CPAP devices Technical Highschool Furtwangen - Germany Prof. Dr. Ing. Bernhard Vondenbusch Steinbeis Transfercentre Biomedical Engineering, 2007 In the present report the major characteristics of n. CPAP generators were investigated and compared to each other -high feeding pressure(85 cm. H 2 O) Высокое поддерживащие давление -high noise (74 -79/102 db. A) Сильный шум -aggresive insp. Flow (jet is directly running into the nostrils ) Аггресивный поток смеси в ноздри Infant Flow – fluidic flip technic (Coanda effect) -low feeding pressure (10 cm. H 2 O) -low noise (62 -68 db. A) -volume reservoir (jet is indirectly running at 90° ) Medijet – all types – Benveniste valve +: Range of prongs (3 vs 6) and masks(1 vs 3) -Bonnets with open back for neurosonography and infusions -Generators (1 disposable vs 1 disposable with changing angle and drug nebulizing port and 2 types of reusable), flexible fixation 81
 CPAP Noise Level Medijet 1000 5 cm H 2 O = 58 db. A Microphone distance 30 cm CPAP Noise Level Infant Flow DB 350 5 cm H 2 O = 72 db. A n 2 = with filter Microphone distance 30 cm
CPAP Noise Level Medijet 1000 5 cm H 2 O = 58 db. A Microphone distance 30 cm CPAP Noise Level Infant Flow DB 350 5 cm H 2 O = 72 db. A n 2 = with filter Microphone distance 30 cm
 Noise levels, Montreux, 2010 83
Noise levels, Montreux, 2010 83
 IF vs Medijet 84
IF vs Medijet 84
 the Medijet active n. CPAP Generator family Medijet 1020 reuse weight > 800 g Medijet 1010 reuse weight < 800 g Medijet 1000 with aerosol drug port 85
the Medijet active n. CPAP Generator family Medijet 1020 reuse weight > 800 g Medijet 1010 reuse weight < 800 g Medijet 1000 with aerosol drug port 85
 For Drug nebulisation together with Medijet MJ 1000 86
For Drug nebulisation together with Medijet MJ 1000 86
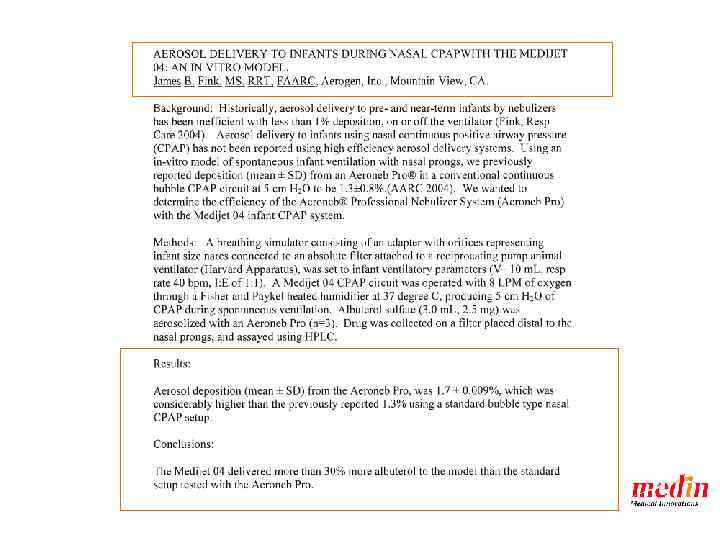
 A Multicenter, Pilot Study of Aerosurf™ Delivered Via Nasal CPAP to Prevent RDS in Preterm Neonates Data presented by Neil Finer’s group PAS San Francisco 88 Привлекательной альтернативой интубации и интратрахеальному назначению сурфактанта может стать аэрозольная доставка сурфактанта. Aerosurf™ • Aerosolized, synthetic, proteincontaining surfactant (lucinactant) • No intubation required for administration, delivered through n. CPAP • Robust KL 4 peptide – Survives the aerosolization process • May significantly expand the clinical utility of surfactants through and beyond the neonatal period доставка сурфактанта при помощи орогастрального зонда в трахею
A Multicenter, Pilot Study of Aerosurf™ Delivered Via Nasal CPAP to Prevent RDS in Preterm Neonates Data presented by Neil Finer’s group PAS San Francisco 88 Привлекательной альтернативой интубации и интратрахеальному назначению сурфактанта может стать аэрозольная доставка сурфактанта. Aerosurf™ • Aerosolized, synthetic, proteincontaining surfactant (lucinactant) • No intubation required for administration, delivered through n. CPAP • Robust KL 4 peptide – Survives the aerosolization process • May significantly expand the clinical utility of surfactants through and beyond the neonatal period доставка сурфактанта при помощи орогастрального зонда в трахею
 89 Neo Mask for n. CPAP and Bronchoscopy Diaphragm
89 Neo Mask for n. CPAP and Bronchoscopy Diaphragm
 90 Application of Surfactant with Bronchoscope F 5, 5 - Mask and Medijet
90 Application of Surfactant with Bronchoscope F 5, 5 - Mask and Medijet
 91
91
 92
92
 93
93

 НРП: • Назальная перемежающаяся принудительная вентиляция, • Аппаратный NCPAP medin applies a certified quality management system in accordance with DIN EN 9001, EN ISO 13485 Annex II section 3 of EG directive 93/42 EEC 95 Lindberghstraße 1, D - 82178 Puchheim +49 (0)89 89 67 09 50 +49 (0)89 80 04 84 76, info@medin-innovations. de :
НРП: • Назальная перемежающаяся принудительная вентиляция, • Аппаратный NCPAP medin applies a certified quality management system in accordance with DIN EN 9001, EN ISO 13485 Annex II section 3 of EG directive 93/42 EEC 95 Lindberghstraße 1, D - 82178 Puchheim +49 (0)89 89 67 09 50 +49 (0)89 80 04 84 76, info@medin-innovations. de :
 96
96
 97
97
 medin - cno Multi–function program 1 2 Flow - 0 -20 l/min CPAP 0 -15 mbar Push Pressure up to 15 mbar Apnoe time 2 to 20 sec Oscillation: Frequencies 5 to 20 Hz cpap apnoe cpap 3 svsp 4 oscillation support ventilation by synchronised pushes medin applies a certified quality management system in accordance with DIN EN 9001, EN ISO 13485 Annex II section 3 of EG directive 93/42 EEC 98 Lindberghstraße 1, D - 82178 Puchheim +49 (0)89 89 67 09 50 +49 (0)89 80 04 84 76, info@medin-innovations. de :
medin - cno Multi–function program 1 2 Flow - 0 -20 l/min CPAP 0 -15 mbar Push Pressure up to 15 mbar Apnoe time 2 to 20 sec Oscillation: Frequencies 5 to 20 Hz cpap apnoe cpap 3 svsp 4 oscillation support ventilation by synchronised pushes medin applies a certified quality management system in accordance with DIN EN 9001, EN ISO 13485 Annex II section 3 of EG directive 93/42 EEC 98 Lindberghstraße 1, D - 82178 Puchheim +49 (0)89 89 67 09 50 +49 (0)89 80 04 84 76, info@medin-innovations. de :
 Program 1 99
Program 1 99
 Program 2 100
Program 2 100
 Program 3 101
Program 3 101
 Program 4 102
Program 4 102
 When in doubt, let the kid make his own damn vent changes!!! Courtney, MD
When in doubt, let the kid make his own damn vent changes!!! Courtney, MD