
1 ASEPSIS AND ANTISEPSIS History of surgery





lecture-01-asepsis-antisepsis-operation.ppt
- Размер: 18.3 Mегабайта
- Количество слайдов: 50
Описание презентации 1 ASEPSIS AND ANTISEPSIS History of surgery по слайдам
1 ASEPSIS AND ANTISEPSIS History of surgery Department Of Surgical Diseases Professor assistant, MD Gennady N. Gerasimov
2 Surgery • Is the branch of medicine, in which various mechanical or physical therapeutic manipulations are used
3 Surgery • The art or practice of treating injures deformities and other disorders by manual operation or instrumental appliances
4 The surgeon /from Clinical Surgery. Of Michael M. Henry London/ • Is one who makes people better chiefly by the exercise of manual skills / Operate first, questions later /. Surgeons have skills in management that go beyond mere manipulative ones and look after many patients who might possibly need an operation
5 Operation?
6 Operation • Is a specific mechanic intervention upon a part of the body for diagnosis and treatment
7 Operation • Urgent – to be performed immediately or within a few hours following the patient’s admission • Emergency – should be done in several days after patient’s admission • Scheduled – if the date of the operation is fixed before patient’s admission
8 Operation • Radical – removes the cause of diseases, or part of organ • Palliative – relieve symptoms of diseases
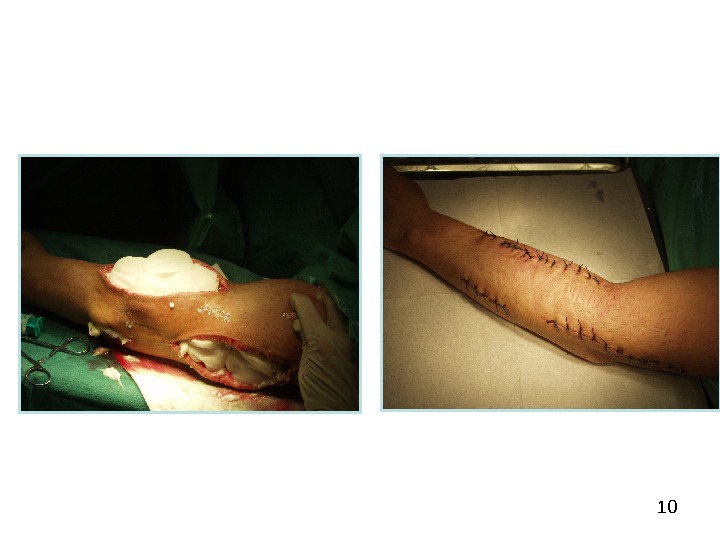
9 • Consist of three steps : • Operative access • Primary step • Finishing the operation, suture of wound Operation
11 History of surgery asepsis
12 Joseph Lister / 1827 – 1912 / • Made one of the great contributions to surgery by demonstrating that antisepsis could prevent infection. In march 1865 he began placing pure carbolic acid into wounds/ reduced concentration to 10, 5 and 2, 5 percent /. In 1867 he published his initial series of papers on antiepsis • In 1871 Lister began to use a carbolic acid spray to reduce contamination of the operating room atmosphere
13 Ernst Bergman /1882/ • Aseptic sugery was not generally practiced. When asked what was new in surgery 1882, Ernst Bergman said, « Today we wash hands befor an operation»
141880 s -1890 s • Sterilization of instruments came into practice, first by chemicals and then by steam • Hand washing and the wearing of masks, caps, gowns and gloves were also introduced about this time • William Stewart Halsted (1852 -1922) introduced rubber gloves for his scrub nurse, Caroline Hampton, because mercuric chloride irritated her skin • Joseph Bloodgood introduced ther routine use by the entire operating t ea m
15 The introductuon of antibiotics • The discovery of penicillin was first reported by Alexander Fleming \ USA\ in 1928, it was not used clinically until administered by Howard Florey in the 1948 s. • In the Soviet Union antibiotics were introduced into clinical practice in the 1940`s by Z V Ermolaeva • Antibiotic therapy was a monumental advance inthe treatment of infections
16 ASEPSIS AND ANTISEPSIS
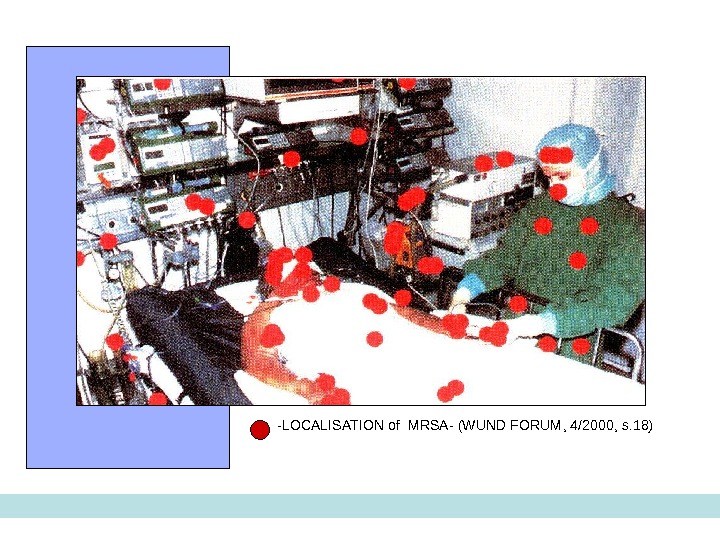
17 — LOCALISATION of MRSA — ( WUND FORUM , 4/2000, s. 18)
18 Condition to make surgical operation • Asepsis — is preventing the infection of wounds and patients • Antisepsis – methods to combat bacterial infection in the wound, patient in surgical department
19 ASEPSIS is preventing the infection of wounds and patients • Nosocamial infection \ all KINDS OF SURGICAL INFECTION\ : 1 Exogenous infection 2 Endogenous infection
20 BASE PRINCIPS OF ASEPSIS • ISOLATION • STERILISATION
21 Exogenous infection • Air born • Drops • Dust • Mixt form • Direct \Pat — Per\ • Indirect \ occupational Patient –Personal —Patient • Suturing material • Prothesis • Contact • Implantional
22 ASEPSIS SURGEON END NURSE • Prophylacxis of dust and drop infection • RULES • Special surgical robe • Special leather shoes • surgical mask • Healthy personal • STOP TALKING in surgical unit • Works requires
Protective glasses Protect the eyes from accidental drops of blood or other fluids. Do not limit the field of view Ensure the absence of refractive effects
24 • Sterilization of the Dressing material • Sterilization of the Surgical Instruments • Sterilization of the Hands and Gloves. ASEPSIS SURGEON END NURSE • Prophylacxis of contact and implantational infections
25 METHODS STERILIZATION OF THE HANDS • Classic method Spasokukotsky-Kochergin : • Running water with soap 10 minutes • Warm 0, 5 per cent ammonium hydroxide solution / 2 x 3 minutes/ • 96 per cent ethyl alcohol/ 2 x 2, 5 minutes • Modern method : With Performic acid Running water with soap 2, 4 per cent solution / 1 minutes / With hibitan, Hibiscrub, Chlorhexidine Running water with soap 0, 5 per cent solution / 3 minutes /
26 METHODS STERILIZATION OF THE HANDS • Modern method : • With Pervomur: /formic acid 85%, 81 ml +hydrogen peroxide 33% 171 ml • Running water with soap – 1 min • 2, 4 per cent solution of pervomur — 1 min • dry with sterile napkin
27 METHODS STERILIZATION OF THE HANDS • With hibitan, Hibiscrub, Chlorhexidine — 0, 5% • Running water with soap- 1 min • 0, 5 per cent solution Hibiscrub, Chlorhexidine / 3 minutes /
28 Mistakes of preparing hands
29 ASEPSIS of students • Prophylacxis of dust and drop infection • RULES • Special surgical robe • Special shoes • surgical mask • STOP TALKING • Works requires
30 Special requirements for students • Students can’t disturb medical personal and patient’s in surgical department • Students can’t speak loudly • Students can’t visit operation room and ward’s without teacher • All information about patient or operation is confidential
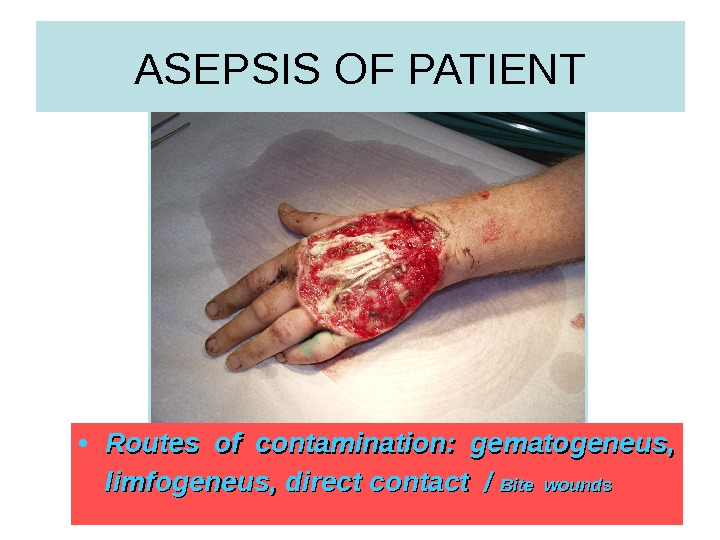
31 ASEPSIS OF PATIENT • Routes of contamination: gematogeneus, limfogeneus, direct contact / Bite wounds
32 ASEPSIS OF PATIENT • Prophylacxis of endogenous infections • Treatment of mouth, skin, focus of infection by Chemotherapy • Prophylacxis of exogenous infections • Preparing of body: desinfection of skin and operative field • Preparing of wound
Micro flora of skin Resident microorganisms from 80% to 90% living on upper layers of skin (natural skin flora) and from 10% to 20% — in deep layers of skin ( in cracks, crypts, hair follicles and the excretory ducts of sweat and sebaceous glands ). Temporary organisms (transient flora, random agents), there are only a limited amount of time and reflect the recent contamination.
IODONATE, povidon-iod • 1 per cent solution for desinfection the OPERATIVE FIELD, DRESSINGS
HYDROGEN PEROXID SOLUTION • 3 PER CENT SOLUTION FOR SKIN, WOUNDS , MUCOUS MEMBRANES
ANTISEPSIS KINDS OF ANTISEPSIS
BIOLOGICAL ANTISEPSIS • ANTIBIOTICS • PROTEOLYTIC ENZYMES • VACCINE • HYPERIMMUNE SERUM • IMMUNOGLOBULINS • IMMUNOSTIMULATORS
Pathogenic microorganisms of surgical infections • gram positive and gram negative • Aerobic and anaerobic
Pathogenic microorganisms • Gram-positive cocci / one of major causative organisms of surgical infections/: staphylococci, streptococci, enterococci, pnrumococci • Gram-positive class / are less important in surgery /: mycobacteria, spirochete, leptospira • Gram-positive anaerobic cocci – peptostreptococci • Gram-positive anaerobic class – clostridium, bifidobacteri
Pathogenic microorganisms • Gram-negative cocci: actinobacter, neisseria • Gram- negative class / often causative organisms of a surgical infections/: E. coli and pseudomonas, klebsiella, enterobacter, salmonella, Helicobacter pylory • Gram-negative anaerobic coccuses — beilonella • Gram-negative anaerobic class – bacteroids, fusobactery
Pathogenic microorganisms • Sensitivity to a drug – is the inhibition growth of microorganism in therapeutic concentrations of antibiotics • Resistance – is the preservation of growth’s ability microorganism in therapeutic concentrations of antibiotics: primary/ before treatment with drug/ or secondary/after treatment with drug/
ANTIBIOTICS • Penicillins: Natural penicillines / benzylpenicilline, bicilline, phenoxymethylpenicilline Antistaphyloccoal – oxacilline, dicloxacine / are active against G+: staphyloccocal infections – pneumonia, lung abscess, osteomyelitis, abscess and phlegmon of soft tissues • Aminopenicillines – ampicilline, amoxycilline combined – ampiox / ampicilline + oxacilline antipseudomonas – carboxypenicilines, aslocilline protected from lactamase – amoxyclav, tasocine / are effective against G-: pseudomonas, proteus – burns, peritonitis
• Cephalosporins • 1 generation/ cefalexinum/ G-, not lactomase activity • 2 generation – cephaloridin, kefsol/ are stable to lactomase, spectrum – G+ and G- microorganisms • 3 generation – cefotaxim, cefaperazon are stable to lactomase, spectrum – G- microorganisms, anaerobic microorganism • 4 generation – cefepin, cefperoson are stable to lactomase, spectrum – G+ and G- microorganisms, anaerobic microorganisms ANTIBIOTICS
• Aminoglycosides –gentamicin, kanamycin, amikacin/ have broad spectrum against G+, G- and anaerobic microorganism • Tetracyclines – tetracycline, rondomicin, vibramicin have broad spectrum against G+, G- and anaerobic microorganism • Macrolides – erytromycin, oleandomycin, azitromycin/ G+, helicobacter • Fluorquinolones – ofloxacin, pefloxacin have broad spectrum against G+, G- and anaerobic microorganism/ E. coli, enterobacteriaceae, klebsiella ANTIBIOTICS
Routes of contamination • Peroral \only in mild infection • Intramuscular \ in most surgical infections • Itravenous \ to achieve high concentration in the blood • Intraarterial \ to achieve high concentration in the blood + short time • Local application
Biologic antiseptic compounds • Proteolytic enzymes can lyse necrotic tissues. Usually used proteolytic enzymes of animal origin are trypsin, chymotypsin, ribonuclease; • those of bacterial origin – terrilitin, streptokinase, collagenase, asperase, ribonuclease, iruxol; • plant origin- papain and bromelain.
IMMUNE STIMULATORS • Improve non-specific immune defence • Prodigiosan \ dificit B lymphocytes\ • Levamisol \ dificit T lymphocytes\
IMMUNIZATION • Active • Staphylococcal anatoxin • Tetanus anatoxin • Passive • Antistaphyloccocal hyperimmune plasma/ of donors` blood/ • Antistaphyloccocal Gamma globulin/ from donor’s blood • Antitetanus serum / from horse’s bloodimmunization
Tetanus / emergency prophylaxis/ • Immunised patients: 0, 5 ml toxoid as a single dose • Non- immunised patients: 1, 0 ml toxoid + 1, 500 -3, 000 IU Antitenanus serum/ 450 -600 IU Antitetanus gamma globulin/ • After 1 month — 0, 5 ml toxoid • After 1 year — 0, 5 ml toxoid
Tetanus • Specific tetanus prophylaxis: 0, 5 ml of toxoid are given twice a month REVACCINATION is done after 1 year — 0, 5 ml of toxoid • Repeaded REVACCINATION after 5 years — 0, 5 ml toxoid`