232885646a4b46987da3a31f12c4d02b.ppt
- Количество слайдов: 37



סוכרת וצום ביום כיפור פרופ' דוד צנגן – מנהל אנדוקרינולוגיה ילדים הדסה

1

2

3

4

5

6

The endocrine and…. exocrine pancreas

β cell signaling

Insulin Signaling

The fasting ability of type I diabetics during religious fasts Reiter J 1, Tsur A 2, Shehadeh N 3, Naveh T 3, and Zangen D 1 1. 2. 3. Department of Pediatrics, Hadassah University Hospital, Hebrew University, Jerusalem. Kupat Holim Klalit, Diabetes Clinic, Jerusalem. Department of Pediatrics, Rambam University Hospital, Technion University, Haifa. Diabetic Medicine 2007 Harefuah 2008 Pediatric Diabetes 2011
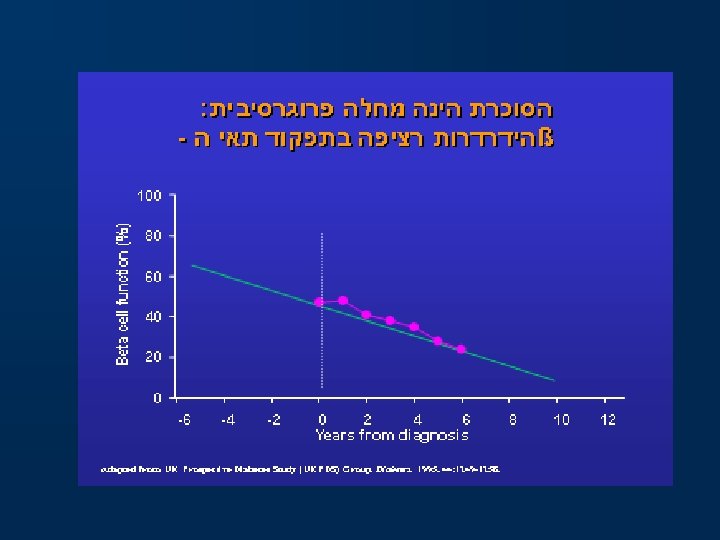
 Diabetic patients have always been advised against fasting on religious fasts: •")
Background (I) Diabetic patients have always been advised against fasting on religious fasts: • Risk of hypoglycemia on insulin 1. • Importance of frequent food intake in diabetics 2. • Possibility of Fasting induced DKA in IDDM 3. 1. 2. 3. Sulimani RA et al: Diabetes mellitus and Ramadan fasting: the need for a critical appraisal. Diabet Med, 1998. Nelson textbook of pediatrics: part XXVI, section 6. Burge MR et al: Short-term fasting is a mechanism for the development of euglycemic ketoacidosis during periods of insulin deficiency. J Clin Endocrinol Metab, 1993.
 Ramadan fasting data: • Type II DM: – 1992 – Beshyah –")
Background (II) Ramadan fasting data: • Type II DM: – 1992 – Beshyah – 1993 – Ahmed – 1998 – Ali – improved control of diabetes 1 – insulin treated 2 – increased hypoglycemic episodes 3 • Type I DM: – 1992 – Salman – 2001 – Kadiri 1. 2. 3. 4. 5. – emphasis on monitoring blood glucose 4 – lispro vs. short acting insulin 5 Beshyah SA et al: Effect of Ramadan fasting on metabolic control in diabetes. Diabet Med, 1992. Ahmed AF et al: Ramadan fasting and insulin dependent diabetes mellitus…Int Diab Digest, 1993. Ali RU et al: Fasting in Ramadan and the diabetic patient (letter). Diabetes-Care, 1998. Salman H et al: Ramadan fasting in diabetic children in Riyadh. Diabet Med, 1992. Kadiri A et al: Treatment of type I diabetes with insulin lispro during Ramadan. Diabetes Metab, 2001.
 Jewish religious fasts: • No documented data. • 25 hour fasts. •")
Background (III) Jewish religious fasts: • No documented data. • 25 hour fasts. • Patients fast against medical advise due to religious and social motives: – Leviticus/23/27 – “ye shall afflict your souls” – 98. 9% of religious, 75. 9% of total Israelis, fast during Yom Kippur. 1 – Eric Erikson – pubertal development etc. 1. The Central Bureau of Statistics 1991

"בעשור לחדש השביעי הזה יום הכיפרים הוא. . . ועניתם את נפשתיכם. . . כי כל הנפש אשר לא תענה בעצם היום הזה ונכרתה ( מעמיה'" )ויקרא כג פסוקים כז-כט “on the tenth day of this seventh month is the day of atonement… and ye shall afflict your souls…for whatsoever soul it be that shall not be afflicted in that same day, he shall be cut off from his people” (Leviticus/23/27 -29)

Aims • To test the ability of diabetic patients to fast 25 hour fasts safely. • To determine the optimal insulin dosing.
 patients : • Type I diabetics aged 12 -40. • Patients -")
Methods (I) patients : • Type I diabetics aged 12 -40. • Patients - who intended to fast in any event. • Patient variables examined : Age, gender, weight, BMI, duration of diabetes, Hb. A 1 C, no. of hypoglycemic episodes per week, daily glucose levels (representative), fasting hypo and hyperglycemia, percent of total daily insulin dosage during the fast.
 The protocol: • Blood glucose monitoring every 2 ½ hours. • Situations")
Methods (II) The protocol: • Blood glucose monitoring every 2 ½ hours. • Situations in which patients should stop fasting: – Nausea or vomiting – stop fasting and consult a physician. – Glucose >350 – indication for fluid intake. – Glucose <79 or symptoms of hypoglycemia – indication for food intake.
 Possible insulin adjustments: • Pre fast Lunch – 2/3 of short acting")
Methods (III) Possible insulin adjustments: • Pre fast Lunch – 2/3 of short acting insulin • Evening (mafseket) - ¾ of short acting insulin • Night - ½ of intermediate acting insulin. • Morning – ¼ of intermediate acting morning insulin (and ¼ of short acting lunch insulin- if regularly administered).
 The patients: • 190 patients were contacted, 39 reports were collected. min")
Results (I) The patients: • 190 patients were contacted, 39 reports were collected. min Gender max F = 22(56%) Mean (med) ± sd M = 17(44%) Age 12 40 18. 36(16) ± 6. 73 Duration of diabetes 2 m 23 y 7. 16(6 y) ± 6. 04 BMI 17. 5 27. 2 21. 25 ± 2. 55 No of hypoglycemic episodes per week Hb. A 1 C 0 5 2. 07 ± 1. 3 5. 7 11. 6 8. 71 ± 1. 48
 fasting Success: USF SF")
Results (II) fasting Success: USF SF
 Comparison of patient subgroups: SF Mean ± sd Gender (%) Age Duration")
Results (III) Comparison of patient subgroups: SF Mean ± sd Gender (%) Age Duration of diabetes Weight BMI USF sig Mean ± sd M 70. 6 M 29. 4 0. 648 F 63. 6 F 36. 4 18. 38 ± 6. 85 18. 31 ± 6. 76 0. 974 6. 8 ± 5. 08 7. 9 ± 7. 87 0. 667 55. 77 ± 10. 12 56. 92 ± 10. 88 0. 761 20. 73 ± 2. 40 22. 28 ± 2. 62 0. 101
 SF Mean ± sd No. of hypoglycemic episodes per week Mean of")
Results (IV) SF Mean ± sd No. of hypoglycemic episodes per week Mean of daily glucose levels (representative) Hb. A 1 C USF Mean ± sd 2. 28 ± 1. 33 1. 77 ± 1. 25 sig 0. 291 159. 5 ± 44. 84 159. 2 ± 50. 03 0. 985 9. 00 ± 1. 55 8. 16 ± 1. 21 0. 124
 * p=0. 041 * p=0. 042 * n=26 * n=13 Average no")
Results (V) * p=0. 041 * p=0. 042 * n=26 * n=13 Average no of fasting hyperglycemic episodes (>350) n=26 n=13 Average no of fasting hypoglycemic episodes (<85)
 *p=0. 049 *p=0. 046 * * n=26 n=13 Percent of total daily")
Results (VI) *p=0. 049 *p=0. 046 * * n=26 n=13 Percent of total daily insulin dosage – from the prefast lunch n=26 n=13 Percent of total daily insulin dosage – from the “mafseket”
 *p=0. 051 * n=26 n=13 Percent of total daily insulin dosage –")
Results (VII) *p=0. 051 * n=26 n=13 Percent of total daily insulin dosage – from bedtime
 Factors that correlated with extreme glucose levels during the fast ( <85")
Results (VIII) Factors that correlated with extreme glucose levels during the fast ( <85 or >350): • 76. 5% of these occurred in females. *p=0. 024 * n=23 n=11 Mean of daily glucose levels
 Comparison of the fast and representative days: • Patients who had glucose")
Results (IX) Comparison of the fast and representative days: • Patients who had glucose levels under 85 on the representative day where at higher risk for similar glucose levels during the fast (p=0. 01). • Patients who had glucose levels above 250 on the representative day where at higher risk for similar glucose levels during the fast (p=0. 01).
 Hyperglycemia is more frequent when fasting: P=0. 481 Values below 85 P=0.")
Results (X) Hyperglycemia is more frequent when fasting: P=0. 481 Values below 85 P=0. 035 Values exceeding 250

המלצות לטיפול ביום הצום טיפול לקראת הצום • ניטור גלוקוז וקטונים בשתן * ללא זריקות במהלך הצום פרט לטיפול בעת היפרגליקמיה. * לערכי גלוקוז מעבר ל 052 מ"ג/ד"ל - הזרקת אינסולין לתיקון ל 051 מ"ג/ד"ל. הפחתת מינון לקראת סעודה שלפני הצום, יש להזריק רק 66 עד %57 ממנה רגילה חולי סכרת סוג 1 - אינסולין לטווח קצר regular insulin או analogue , insulin, novorapidra, , humalog * ערכי גלוקוז מעבר ל 053 מ"ג/ד"ל – יש להפסיק לצום להזריק אינסולין ולשתות * יש להפסיק לצום במקרה של היפוגליקמיה )מתחת ל 08 מ"ג/ד"ל ( הפחתת מינון ל-%05 מהמינון הרגיל בליל הצום אינסולין לטווח בינוני/ארוך Long acting analogue ) insulin (lantus, levemir *הורדת קצב בזאלי ל %05 מהרגיל * ללא זריקות נוספות פרט לזריקות לצורך תיקון היפרגליקמיה כמתואר * ניטור גלוקוז וקטונים בשתן להפחית את מנת האינסולין בסעודה מפסקת ל %57 -66 ממנה רגילה משאבת אינסולין

טיפול בצום * אין ליטול תרופות אלו בצום * ניטור גלוקוז * הפסקה בעת היפוגליקמיה טיפול לקראת הצום אסור לצום או לשנות את הטיפול ל 3 repaglinide ימים לפני הצום שם גנרי )מסחרי( חולי סכרת מסוג 2 מטופלים בתרופות Chlorprpamide ) (Diabitex סולפונילאוראה דור 1 * אין ליטול תרופות אלו בצום לקיחה רגילה של התרופה לפני סעודה מספקת. Tolbutamide ) (orsinon * אין ליטול תרופות אלו בצום. פעם 1 ביום - לקחת מינון רגיל בארוחה לפני הצום Glibenclamide ) (Gluben, Glibetic *ניטור גלוקוז 2 פעמים ביום- להפחית לחצי מנה בארוחות ביום לפני הצום ) Glipizide (Glucorite * ניטור גלוקוז * הפסקה בעת היפוגליקמיה *הפסקת צום בהיפוגליקמיה הערה- תרופות נוספות לסכרת, -warfarin, Salicylates סכנהלהיפוגליקמיה 3 פעמים ליום- * לא לצום *או להפחית את המינון לחצי ביומיים לפני הצום * או לעבור ל repaglinide יומיים לפני הצום סולפונילאוראה דור 2

• אין ליטול תרופות אלו בצום • הפסקת צום בעת היפוגליקמיה • אין ליטול תרופות אלו בצום *הפסקת צום בעת היפוגליקמיה ליטול מנה רגילה לקראת ארוחה לפני צום Acarbose ) (Prandase Repaglinide ) (Novonorm Alpha glucosidase inhibitors Meglitinides Rosiglitazone , (Avandia ) Rossini Thiazolidinedi ones Metformin , (Glucophage , Glucomin ) Glufor Biguanides
 • 2/3 of the fasters were successful. • Patients with blood glucose")
Summary (I) • 2/3 of the fasters were successful. • Patients with blood glucose levels above 350 or below 85 stopped fasting. • Successful fasters took an average of a 1/3 of their total daily regular insulin dosing. A further decease is advised for the night dose. • Females and patients with higher mean glucose levels during regular days had more extreme values during the fast.
 • Extreme glucose levels during weekdays predicted similar glucose levels during the")
Summary (II) • Extreme glucose levels during weekdays predicted similar glucose levels during the fast. • High blood glucose levels are more frequent during the fast, low levels are not.

conclusions • 25 hour fasting may be successful and safe. • A third of the total daily insulin dosage is recommended during the fast. A further decease is advised for the night dose. • Since high glucose levels are encountered vigorous monitoring is mandatory. • Extreme week day glucose levels and woman are at greater risk for extreme glucose levels during the fast.

Peditric Endocrine Unit David Gillis Ishaya Wexler Abdulsalam Abu Libdeh Adi Orbach , Najwa abed el hak Eran Lavi Maha Abdulhadi-Atwan Omar Maali , Mahmoud Zigan Moria Barkasa Jessica Leibovitz Shoshana Palmor Patients and families Institute of Genetics –Shaare Zedek Hospital Efrat Levy Lahad Paul Renbaum Ariella Weinberg Shukrun Israeli Pediatric Endocrine Units Yardena Tenenbaum-Rakover (Haemek - Afula) Mariana Rachmiel (Assaf Harofeh) Dep. Of Cellular Biochemistry and Human Genetics And Developmental Biology – Hebrew University Medical School-Jerusalem Offer Gerlitz Rachel Khalifa Amtzia Dreifuss Tiqva Shorr Institute of Medical Genetics- Seattle Mary-Claire King Funding: The Israel Science Foundation (ISF) The US Agency for International Development (USAID) program for Middle East Regional Cooperation
232885646a4b46987da3a31f12c4d02b.ppt