63319224879430d5011acc82ac69e46e.ppt
- Количество слайдов: 84



מתוק, מתוק יותר, מתוק מידי סוכרת 2002 חידושים ועידכונים דר' אילנה הרמן-בהם מרכז רפואי אוניברסיטאי סורוקה

DIABETES A MAJOR GLOBAL HEALTH PROBLEM REQUIRES AN URGENT EFFECTIVE GLOBAL SOLUTION

Incidence of Diabetes: New Cases of Diabetes n n n U. K- every 10 minutes Europe - every 40 seconds U. S. A- Every 20 seconds In Israel there are 400, 000 people with diabetes!!!! 10% of the population over age 30!! Ian Campbel, EASD Hypertension Study Group, April, 2001

Diabetes in Adults Is Now a Third World Problem n n n An epidemic of diabetes is occurring throughout the world This trend is strongly related to life-style and socioeconomic change Populations in developing countries and the minority or disadvantaged communities in the industrialized countries now face the greatest risk King H, Rewers M. Bull World Health Org 1991; 69(6): 643 -648.

THE CAUSES OF THE PANDEMIC n n n Migration- the “melting pot” Socioeconomic change- “internal migration” Globalization- the technological revolution

 Carbohydrate gm Heinemann, et al. Diabetic Medicine, 1996; 13: 625")
Pizza Coca-Cola® Tiramisu (dessert) Carbohydrate gm Heinemann, et al. Diabetic Medicine, 1996; 13: 625 -629 140 Energy content k. J 4254 (1017 kcal)

THE BEDOUIN DATA FROM RAHAT 2000 BMI in women aged 35 -44 is 31 Dr. Yunis Abu-Rabiah, Rahat Clinic. Unpublished data

סוכרת בקרב יוצאי אתיופיה n n באתיופיה שיעור סוכרת נמוך - %6. 0 שיעור סוכרת מיד לאחר עליה ארצה: ]רובינשטיין[ n n עליית משה-. %4. 0 , עליית שלמה- %0 לאחר 4 שנים מעלייה %9. 8 ]כהן[ לאחר 7 שנים מעליה , %6. 9 %4. 51 - ] , IGT תורג’מן[

THE THRIFTY PHENOTYPE/ GENOTYPE n n n Poor fetal and infant nutrition are detrimental to the development of beta cells and insulin-sensitive tissues Defective insulin action in utero results in decreased fetal growth Obesity-induced diabetes occurs as a result in later childhood or adulthood

? אז מה רע בקצת סוכר n n n n n 60% hypertension 80% obese 50% lipid abnormalities 2 -4 times more cardiovascular disease and mortality 60% neuropathy Leading cause of blindness Leading cause of renal failure Leading cause of lower limb amputations $$$$$$$$$$

Diabetes is Costly Direct Cost per Year Hypertension $$$$ Diabetes $$$$ Alzheimer's $$$ Schizophrenia $$ Urinary Incontinence $ Chronic Obstructive $ Pulm Disease Congestive Heart $ Failure Osteoporosis $ Post Myocardial $ Infarction HIV $ $ Initial Therapy Acute Complications Chronic Complications Years Health economics support therapeutic innovation Decision Resources, "Decision Base--Final Report", Vols. II-X.

סוכרת טיפוס 2 האם ניתן למנוע את המחלה?

Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle Among Subjects With Impaired Glucose Tolerance n n 225 חולים עם 172 -IGT גברים, 053 נשים: גיל ממוצע 55 , BMI ממוצע 13 הדרכה אישית לירידה במשקל)<%5(, הורדת שומן )>%03(, הורדת שומן רווי )>%01(, תוספת סיבים )<51גר' ליום( ופעילות גופנית )03 דק' ליום( מעקב 2. 3 שנים דיאטנית 7 פעמים בשנה ראשונה אח"כ 4 פעמים בשנה

Results study Wt loss DM Annual incidence at 2 years 3. 5+5. 5 11% 3%/year control 0. 8+4. 4 23% Per personyears 32/1000 6%/year 78/1000
%45 נשים, %46")
2 - Results n n %85 ירידה בסיכון לפתח סוכרת )%45 נשים, %46 גברים( יחס הפוך בין השגת יעדים והופעת סוכרת: %52 יעד סיבים, %68 יעד פעילות אפילו אם יעד משקל לא הושג, השגת יעד פעילות– 0. 2 RR לעומת 6. 0 בביקורת צריך לטפל ב 22 חולי IGT לשנה או 5 ל 5 שנים למנוע מקרה סוכרת 1

Reduction in the Incidence of Type II Diabetes with Lifestyle Intervention or Metformin Diabetes Prevention Program Research Group, The New England Journal of Medicine, Vol. 346, February 7, 2002

Reduction in the Incidence of Type II Diabetes with Lifestyle Intervention or Metformin Diabetes Prevention Program Research Group, The New England Journal of Medicine, Vol. 346, February 7, 2002

Study objective The study was designed to answer three primary questions: Ø Does a lifestyle intervention or treatment with metformin prevent or delay the onset of diabetes? Ø Do these two interventions differ in effectiveness? Ø Does their effectiveness differ according to age, sex, or race or ethnic group?

American Diabetes Association 1997 diagnostic criteria of DM Methods Symptoms of diabetes plus casual plasma glucose concentration 200 mg/dl Impaired glucose tolerance n Randomized clinical intervention trial involving or 2 h plasma glucose 27 centersmg/dl after OGTT were 3234 persons at = 140 – 199 in the US, who at Fastingrisk forglucose 126 mg/dl high plasma diabetes. or All participants gave written informed consent. Impaired fasting glucose n 2 h plasma glucose 200 mg/dl 2. 8 years (1996 -2001). Average follow-up was after OGTT Fasting plasma glucose = 110 – 125 mg/dl (75 g oral n Eligibility criteria: load) n n n Age > 25 BMI > 24 (in Asians > 22) Fasting glucose concentration = 95 – 125 mg/dl 2 h after 75 g oral glucose load = 140 – 199 mg/dl.

Interventions lifestyle modification Three intervention groups: Goal: lifestyle recommendations + 1. Standard achieve and maintain a weight reduction Standard lifestyle recommendations weight. of at least 7% of initial body metformin (Glucophage) 850 mg x 2. § Written information. low-fat diet. • Low-calorie, 2. Standard lifestyle recommendations + § placebo twice daily. (moderate intensity – eg. Brisk Annual 20 -30 min individual session that • Physical activity emphasized the importance of a min per lifestyle. walking) of at least 150 healthy week. 3. Intensive program of lifestyle modification. • A 16 -lesson curriculum covering diet, exercise, and 4. Troglitazone. behavior modification. in 1998 because of Discontinued Liver toxicity * Assignments to metformin and placebo were double-blinded. • Individual sessions to reinforce the behavioral * The study design follow the intention-to-treat principle. changes.

Outcome measures n n The primary outcome was diagnosed diabetes (according to ADA 1997 criteria; confirmation by a second test after 6 weeks). Follow-up included: n n Annual OGTT or semiannual FPGT. Annual measurement of Hb. A 1 c. Annual weight measure. Adherence to interventions was checked by annual questionnaires.

Results

Changes in body weight Leisure physical activity Adherence to medication regimen P value <0. 001 for each comparison

P value <0. 001 for each comparison

Fasting plasma glucose concentrations Hb. A 1 c values

Discussion and conclusions n n n The incidence of diabetes was reduced by 58% with the lifestyle intervention and by 31% with metformin, as compared with placebo. These effects were similar in men and women and in all racial and ethnic groups. The study was not designed to test the relative contributions of each component in the lifestyle intervention.

Discussion and conclusions n n n The estimated number of persons who would need to prevent one case of diabetes is 6. 9 for the lifestyle intervention and 13. 9 for metformin (CI=95%). The effect of metformin was greater with a higher BMI or a higher fasting glucose concentrations. The advantage of the lifestyle intervention over metformin was greater in older persons and those with lower BMI.

Stop NIDDM n n 8141 IGT מטופלים ב 100 Prandase מג 3 X לעומת אין-בו מעקב להתפתחות סוכרת במשך 9. 3 שנים %31 פחות סוכרת בקבוצת מחקר לעומת בקרה

מסקנות n ניתן למנוע הופעת סוכרת טיפוס 2 על ידי: שינוי באורח חיים METFORMIN PRANDASE

איתור החולה בסיכון לפתח סוכרת n n גורמי סיכון: סיפור משפחתי, השתייכות עדתית, BMI יתר לחץ דם, דיסליפידמיה רמת סוכר בדם בטווח ה IGT, IFG

חינוך למניעה n n חובת ההדרכה לאורח חיים בכל חולה בסיכון גבוה המלצה למעקב ולשקול טיפול תרופתי מונע

סוכרת טיפוס 1 האם ניתן למנוע את המחלה?

772 DIAPEP n n n 53 חולים 1 new onset type מחציתם: 3 זריקות אין-בו או 772 p בזמן 0, חודש ו 6 חודשים 13 סיימו 01 חודשי מעקב 3571 -9471: 853; 1002 Raz et al. Lancet
62. 0")
Results n n בתום 01 חודשים: רמת c-peptide גבוהה יותר מהביקורת )62. 0 nmol/l בביקורת-39. 0 בטיפול( תצרוכת אינסולין נמוכה יותר)76. 0 יחידות לקג' בביקורת- 34. 0 בטיפול( כל החולים מאוזנים טוב מסקנה: שמירה על תפקוד הלבלב ע"י שינוי בהפרשת ציטוקינים

ואם לא ניתן למנוע את הופעת המחלה יש למנוע את הסיבוכים על ידי. . . איזון מרבי n n n של סוכר בדם ערכי לחץ דם שומני הדם וכולסטרול

UKPDS n n n שיפור האיזון מקטין הסיכון לסיבוכים %52 הפחתה בסיכון לסיבוכים מיקרו- ווסקולרים %61 הפחתה בסיכון לאוטם ירידה של %1 ב Hb. A 1 c תביא לירידה של %53 בסיכון

הורדת ל. ד. סיסטולי ב 01ממ' מפחיתה n n CVA ב%44 אי ספיקת לב ב%65 מוות מסוכרת ב%23 סיבוכים מיקרו-וסקולריים ב%73

Goals of Therapy n n n Hb. A 1 c 6. 5 -7% FPG<110 mg% PPG 140 mg% B. P<130/85 mm LDL<100 mg% TG<150 mg%

: סוכרת מסוג 2 הנה שילוב של שני גורמים רגישות היקפית לאינסולין, הפרשה לבלבית של אינסולין Insulin Secretion High Normal glucose tolerance 95 th IGT 50 th Low 5 th Type 2 diabetes Resistant Sensitive Insulin Sensitivity Adapted from Kahn, et al. Diabetes. 1993; 42: 1663 -1672, with permission.

לטיפול יעיל בסוכרת לכן נדרשים. . . n n n שיפור הרגישות לאינסולין הפחתת העמידות לאינסולין הגברת השחרור של אינסולין והתאמתו לצרכים

הכלים n n פעילות גופנית אכילה נכונה תרופות פומיות אינסולין

New Insulin Sensitizers

THIAZOLIDINEDIONES n n n PPARg agonist muscle , fat tissue, liver hepatic metabolism, inactive metabolites excreted in urine single daily dosing monotherapy or in combination with other drugs

Peroxisome proliferator (activated receptors (PPARs Members of the nuclear receptor superfamily of transcription factors Bind to DNA as heterodimers with RXR n Ligand PPARa 83% n DNA 68% PPARg 86% 70% PPARd l Activated by dietary fatty PPAR RXR acids l Regulate genes involved in fatty acid metabolism +/- Willson et al (2000)

EFFECTS AND SIDE-EFFECTS n n n n Decreased triglyceride decreased blood pressure decreased insulin resistance weight gain fluid retention, edema, CHF increased LDL dilutional anemia liver impairment
: complementary mode of action to metformin and SU Rosiglitazone improves b-cell function")
Rosiglitazone (AVANDIA): complementary mode of action to metformin and SU Rosiglitazone improves b-cell function – a key factor in disease progression Pancreas Sulfonylureas primarily work by increasing insulin release from the pancreas Rosiglitazone decreases excessive lipolysis and reduces free fatty acid output Rosiglitazone decreases excessive hepatic glucose production Metformin primarily works by reducing glucose output from the liver Adipose tissue Muscle Liver Rosiglitazone directly reduces insulin resistance – a key underlying factor in type 2 diabetes
 הפרשת האינסולין בסוכרת ובבריאים 800 Normal Type 2 DM 700 600")
Insulin Secretion (pmol/min) הפרשת האינסולין בסוכרת ובבריאים 800 Normal Type 2 DM 700 600 500 400 300 200 100 0600 1000 1400 Polonsky et al. New Eng. J. Med. 1996; 334 1800 Time 2200 0600

REPAGLINIDE הטבליה הראשונה מקבוצת PPG Regulators – ה
 800 700 Normal")
עקומות הפרשת האינסולין בסוכרתיים, בבריאים ובמטופלים בנובונורם Insulin Secretion (pmol/min) 800 700 Normal Type 2 DM 600 Novo. Norm 500 400 300 200 100 0600 1000 1400 1800 Time 2200 0600 Polonsky et al. New Eng. J. Med. 1996; 334

אנלוג אינסולין מהיר פעולה d Novo. Rapi

מתכונת הטיפול באינסולין כיום אינסולין פרמקולוגי 06 ארוחות 05 זמן הזרקות 04 03 ) Insulin (m. U/l רמות אינסולין בבריאים 07 02 01 0 0060 0030 0042 0012 0081 0051 0021 0090 0060 Time of day NPH ערב צהרים בוקר 8891. Adapted from Polonsky et al
 (pmol/l 005 אינסולין נובורפיד אינסולין הומני")
פרופיל האינסולין של נובורפיד באנשים בריאים ) (pmol/l 005 אינסולין נובורפיד אינסולין הומני קצר טווח זמן הזרקה 054 ) (m. U/l 57 004 003 052 002 051 Serum insulin 053 52 001 05 0 006 045 084 024 063 003 042 081 021 06 0 0 06 - ) Time (minutes 6991. Adapted from Heinemann et al

INSULIN LISPRO ® Humalog
 INSULIN LISPRO Serum Insulin Levels (ng/ml) After Subcutaneous Injection in")
Serum insulin levels (ng/ml) INSULIN LISPRO Serum Insulin Levels (ng/ml) After Subcutaneous Injection in Healthy Volunteers ( N=10 ) 5 4 Humalog® Humulin® R 3 2 1 0 0 1 12 2 3 Howey DC et al. Diabetes 1994; 43: 396 -402. 4 5 6 7 Time (Hours) 8 9 10 11


Inhaled Insulin n n n חלקיקים קטנים המגיעים ל alveoli 4 מחקרים: 3 אבקה, אחד נוזל שיא תוך שעה, טווח פעולה 4 שעות- בדומה לאנלוגים ניתן להשתמש גם ב ULTRA, NPH אין השפעה על תפקודי ריאות בטווח הקצר סה"כ %02 -31 ספיגה מינונים גבוהים

Inhaled Insulin n n ספיגה ויעילות הורדת רמת סוכר בצום ואחרי אוכל כמו בהזרקה תת-עורית אין יותר מאורעות היפוגליקמיה אין גירוי בדרכי הנשימה אין ירידה בתפקודי ריאות יעיל גם בטיפוס 1 וגם בטיפוס 2

Inhaled Insulin n n הבעיות: המיכשור למתן האינסוליין-גדול, מסורבל רק כ%02 -%01 נספג לריאות כמות האינסולין הגדולה מידת הספיגה במחלת ריאות? השפעות ריאתיות לטווח ארוך?
 Insulin")
מתכונת הטיפול באינסולין כיום אינסולין פרמקולוגי ארוחות 06 05 04 03 ) Insulin (m. U/l רמות אינסולין נורמליות 07 02 01 0 0060 0030 0042 0012 0081 0051 0021 0090 0060 Time of day NPH ערב צהרים בוקר 8891. Adapted from Polonsky et al
 A long acting insulin analogue")
LANTUS® (insulin glargine) A long acting insulin analogue

The Ideal Long Acting Insulin n n n 1 injection daily covers 24 hours no peaks or peaks at the correct time safe n no toxic effects n no mitogenic effects n no immunogenic effects low intrasubject and intersubject variability easy handling n injection at different sites n injection at different times n no mixing necessary good glycemic control high treatment satisfaction and acceptance

Basal-Bolus regimen using Lantus to simulate basal insulin secertion Modified concept of intensified conventional therapy 7. 00 12. 00 19. 00 22. 00 Intensified conventional therapy using HOE 901 for basal insulin substitution 7. 00 12. 00 19. 00 22. 00

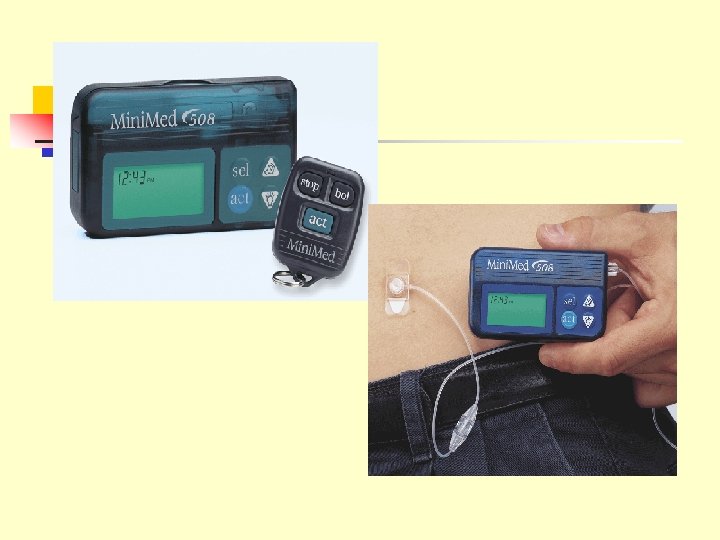
משאבת אינסולין למי ומתי?

מעקב – תפקיד החולה כל יום: בדוק רמת סוכר 4 -6 פעמים ביום ותמיד לפני השינה. עקוב על פי ההנחיות לטיפול בהיפוגלוקמיה. כל חודש: אם היו: DKA לסקור ארועי בדוק סוכר בשלוש לפנות בוקר לבדוק סוכרים יממה שלמה שעה ו/או שעתיים אחרי האוכל

אינדיקציות לטיפול במשאבה גבוה HGAIC היפרגליקמיות חוזרות אפקט השחר סוכר גבוה בבוקר פעילות גופנית ילדים הריון גסטרופרוזיז סגנון חיים לא מסודר עבודה במשמרות עמידות לאינסולין TYPE II

השלכות כלכליות עלויות – החזר קופות החולים – %09 המשאבה כלולה בסל השירותים צורך התחלתי בחינוך והדרכה עלות המתכלים/ חודשי

סיכום הטיפול במשאבה הנו הטיפול הקרוב ביותר למנגנון הפיזיולוגי של הפרשת האינסולין. המוניטור מספק למשאבה עוצמה טיפולית ודיוק.

Summary For most patients, starting insulin pump therapy is an extremely positive lifechanging experience

טיפול אינטנסיבי באינסולין הוריד תמותה לאחר אוטם שריר הלב בחולי סוכרת Standard treatment IV Insulin 48 hours, then 4 injections daily. 7 All Subjects . 7 . 6 (N = 620) Risk reduction (28%) P =. 011 . 6 . 5 Low-risk and Not Previously on Insulin (N = 272) Risk reduction (51%) P =. 0004 . 5 . 4 . 3 . 2 . 1 0 0 0 1 2 3 4 Years of Follow-up DIGAMI, BMJ, 1997: 314: 1512 -15 5 0 1 2 3 4 Years of Follow-up 5

טיפול אינטנסיבי באינסולין בחולים ב - ICU הפחית תמותה ותחלואה באופן משמעותי 8451 חולים לא סוכרתיים, המאושפזים לאחר ניתוח בטיפול נמרץ, טופלו באינסולין להורדת היפרגליקמיה לערכים נורמוגליקמים : % 110 -80 mg 1002 , 8 Greet V. D. B at all: NEJM, 345, 19. November

טיפול אינטנסיבי באינסולין הפחית את אחוזי התמותה בחולים מונשמים בכל דרגות החומרה : APACHE II מדד של חומרת המצב הפיזיולוגי החריף והערכת מצב בריאותי מתמשך. גבוה יותר = חמור יותר 1002 , 8 Greet V. D. B at all: NEJM, 345, 19. November

סיכום n קיימת מגפה של סוכרת ואיתה תחלואה ותמותה גבוהים n סוכרת טיפוס 2 ניתנת למניעה n איזון הסוכרת מונע סיבוכים ותמותה גם במצב החריף וגם לטווח הארוך n קימות תרופות וטכנולוגיות יעילות לטיפול יש להיעזר בהם על מנת להשיג את יעדי האיזון
63319224879430d5011acc82ac69e46e.ppt