
Trauma in Childhood. Initial assessment and management. Травма



:")




 has")







 immunisation; (2)")





14872-1._trauma.ppt
- Количество слайдов: 32
Trauma in Childhood. Initial assessment and management. Травма у дітей. Екстрена медична допомога невідкладних станів
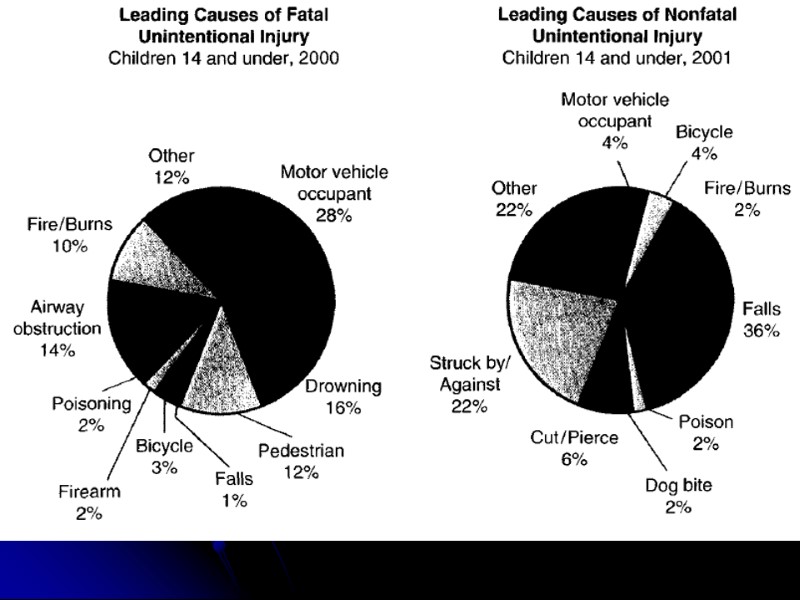
There are three ways to lessen or prevent childhood injury 1 Education of parents and children about potential accident situations. 2 Minimisation of injury in the actual accident, for example, use of car restraints or cycling helmets. 3 Limitations of injuries sustained after the accident, for example, by fi rst aid techniques. This requires an effective transport system, which allows early, accurate assessment of injuries by trained personnel and rapid resuscitation prior to transport to an appropriate institution.
The ‘trimodal distribution’ of trauma death was first described in 1983: 1 Immediate (minutes): major vascular or neurological insult. 2 Early hours (‘golden hour’; 1–2 h post injury): 35% of deaths, secondary to brain, abdominal or chest injury. 3 Late (days to weeks): 15% of deaths, from brain death, multiorgan failure and/or overwhelming sepsis.
Establishing priorities The Early Management of Severe Trauma course (instituted by the Royal Australasian College of Surgeons) has developed a set of priorities, which apply to adults and children. In summary, patient management consists of a rapid primary survey and resuscitation of vital functions, followed by a more detailed secondary assessment; then stabilization and transfer to definitive care centre.
The primary survey: ‘A, B, C’s’ During the primary survey, life-threatening conditions are identified and treatment instigated immediately: 1 A – Airway maintenance with cervical spine control. 2 B – Breathing and ventilation. 3 C – Circulation with haemorrhage control. 4 D – Disability: neurological status. Do not forget the glucose. 5 E – Exposure and environmental control
Circulation Children will compensate for hypovolaemic shock with tachycardia and vasoconstriction. Hypotension will not occur until more than 30% of circulatory volume is lost. Hypotension is a preterminal sign in paediatrics. Note: Tachycardia may be a response to fear and pain or a normal anxiety response.
Exposure and environmental control The patient should be completely undressed, usually by cutting off the garments. It is imperative to cover the patient with warm blankets to prevent hypothermia in the emergency department. Intravenous fluids should be warmed and a warm environment maintained. Patient privacy should be maintained.
Secondary survey The secondary survey begins after the primary survey (A, B, C) has been completed, and the resuscitation phase (management of other life-threatening conditions) has begun. It is a comprehensive examination top-to-toe and front-to-back (including log roll) examining all orifices, with full documentation of all injuries with instigation of first aid management. Ensure that you explain to the child and carers what you about to do and keep the child warm during exposure. In paediatrics a rectal and vaginal examination are not routine and should only be performed once if deemed necessary by the appropriate specialist.
Monitoring • Ensure continuous monitoring of all parameters. If any changes occur the primary survey should be repeated.
Superficial soft tissue injuries The extent and severity of soft tissue injuries tend to be underestimated. It is important to take into consideration the mechanism of injury, that is, high velocity/penetrating/is there a high risk of contamination? The initial first aid management of any wound is irrigation and cleaning – sterile water will suffice.
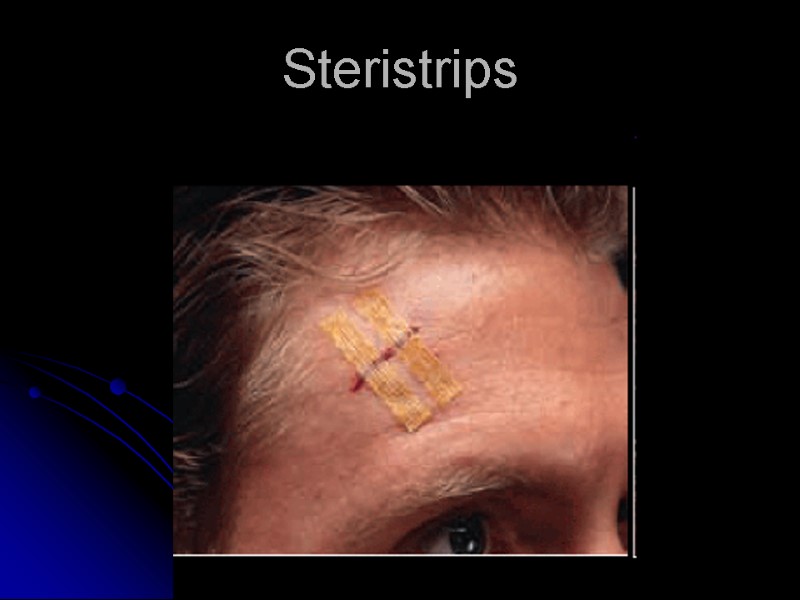
Wound closure Superfi cial wounds can be cleaned and managed with a simple dressing. Simple small lacerations that are not under tension can be closed with either – a tissue adhesive ‘Dermabond glue’ or adhesive strips ‘steristrips’. Other wounds will require surgical closure with sutures.
Steristrips
Specific injuries The tongue Despite initially vigorous bleeding and major deformity of the tongue contour, suture of the tongue is rarely needed. Most lacerations should be left to heal and remodel naturally. Infection of intraoral lacerations is rare. Consider referral to specialist for review if there is a full thickness injury or if there is a large flap.
The straddle injury A slip on to the edge of the bath, bicycle bars or a fence may cause injury to the perineum. Where adequate assessment is not possible in the emergency room, children should be admitted for examination and definitive management under anaesthesia. In females, a straddle injury often causes a tear in the posterior fourchette, often with significant bleeding; minor splits do not require sutures. Injuries through the hymen need careful repair. Where a laceration has penetrated into the rectum, a colostomy for faecal diversion is required. In boys, a straddle injury may tear the bulbar urethra and cause extravasation of urine into the scrotum and lower abdominal wall. A urethrogram demonstrates leakage of contrast and the need for catheter drainage of urine or primary urethral repair.
Antibiotics The most important factor in the prevention of infection is in the use of primary first aid and cleaning and if necessary surgical debridement of extensive wounds. Antibiotics should be used when wounds are contaminated, but antibiotics are ineffective in the presence of dead tissue or foreign matter, and should never be relied upon to prevent infection in contaminated wounds.
Tetanus Successful prophylaxis against clostridial infections rests upon the triad of: (1) immunisation; (2) antibiotics and (3) adequate surgical cleansing of wounds: removal of dead tissue, foreign material and blood clot.
Active immunisation Tetanus immunisation should be part of routine childhood immunisation. Primary immunisation of infants is achieved with three doses of triple antigen (diphtheria, tetanus, pertussis) and booster doses at 4 and 15 years. The new vaccination schedule recommends that the 1-yearly tetanus booster is no longer required up until the age of 50 years, provided the primary series of three vaccinations plus two boosters has been given. It is important to be aware of the current schedule of childhood immunisations.
Passive immunisation Tetanus immunoglobulin is available for the passive protection of individuals who have sustained a tetanus-prone wound, and those who have received less than three doses of tetanus vaccination.
Homework APLS Advanced paediatric life support the practical approach ATLS Advanced Trauma Life Support Jay. L. Grosfeld - Pediatric Surgery 2-Volume Set - 2006. 265-274