
Pericardial disease Pericardium • Visceral













- Размер: 7.3 Mегабайта
- Количество слайдов: 35
Описание презентации Pericardial disease Pericardium • Visceral по слайдам
Pericardial disease
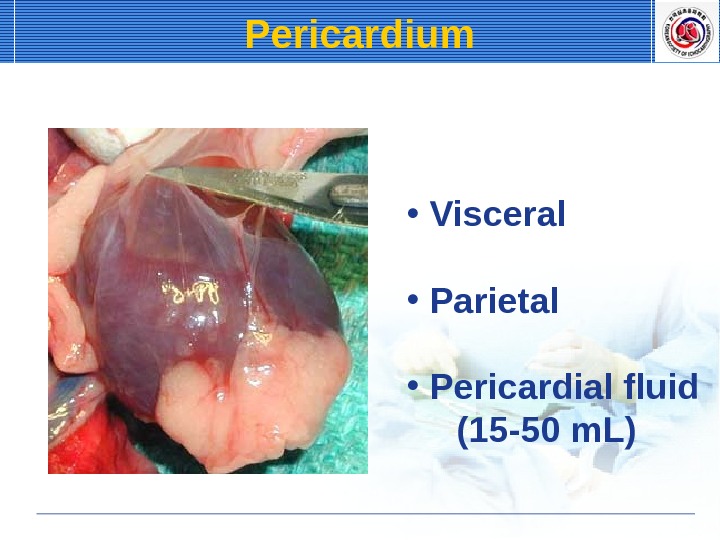
Pericardium • Visceral • Parietal • Pericardial fluid (15 -50 m. L)
Role of Echo Identify pericardial effusion / thickening Characterize hemodynamics — RV diastolic collapse — Doppler filling patterns (tamponade vs constriction) Guide pericardiocentesis
Pericardial effusion Normal: 20 -30 ml Clinical manifestation nonspecific, muffled heart sound CXR: cardiomegaly ECG: low voltage, electrical alternans Echocardiography: accurate, quick Diagnostic pericardiocentesis 시시시시시 시
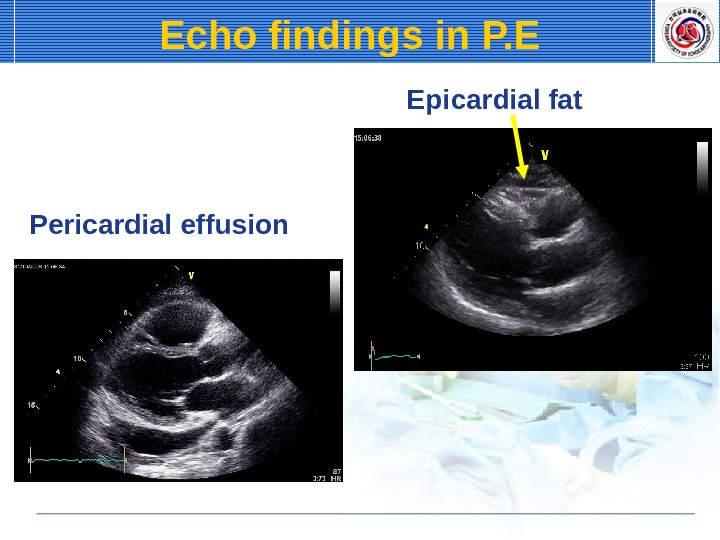
Echo findings in P. E Normal Pericardial effusion
Pericardial effusion Pleural effusion. Echo findings in P.
Epicardial fat. Echo findings in P. E Pericardial effusion
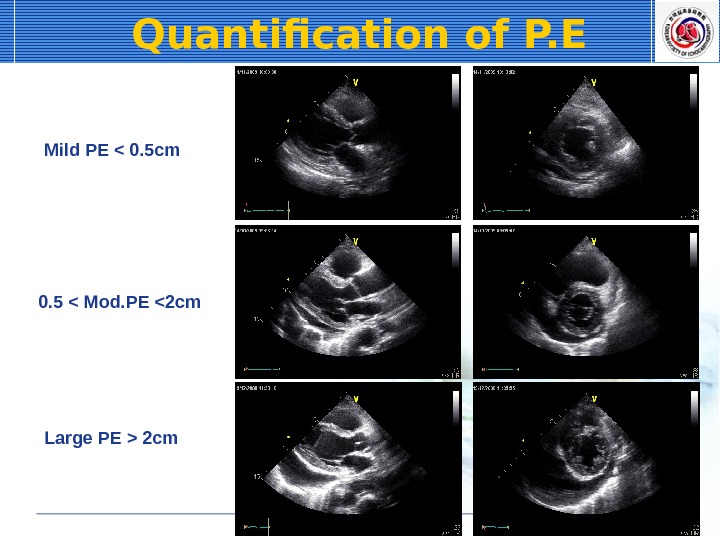
Quantification of P. E Mild PE < 0. 5 cm 0. 5 < Mod. PE 2 cm
Acute Pericaridtis Inflammation of pericardium Clinical diagnosis Pericardial effusion or pericardial thickening
Etiology of Pericardtis Infectious: viral, pyogenic, Tbc, fungal Noninfectious: AMI, uremia, neoplasia, myxedema, trauma, aortic dissection, radiation Immunologic rheumatic, collagen vascular disease, drug, postcardiac injury
Chest pain acute infectious, immunologic etiology retrosternal, right precordial referred to back, trapezius aggravated by inspiration, coughing relieved by sitting up and leaning forward Dyspnea Systemic Sx: fever, weight loss. Symptoms of pericarditis
Pericardial friction rub sitting up, high-pitched, scratching, to-and-fro sound ECG widespread ST elevation (AMI 시 시시시 !) no QRS changes, no reciprocal change T wave inversion after days CXR: normal Echo. CG: normal or pericardial effusion. Clinical findings of Acute pericarditis
Electrocardiogram. Acute Pericarditis
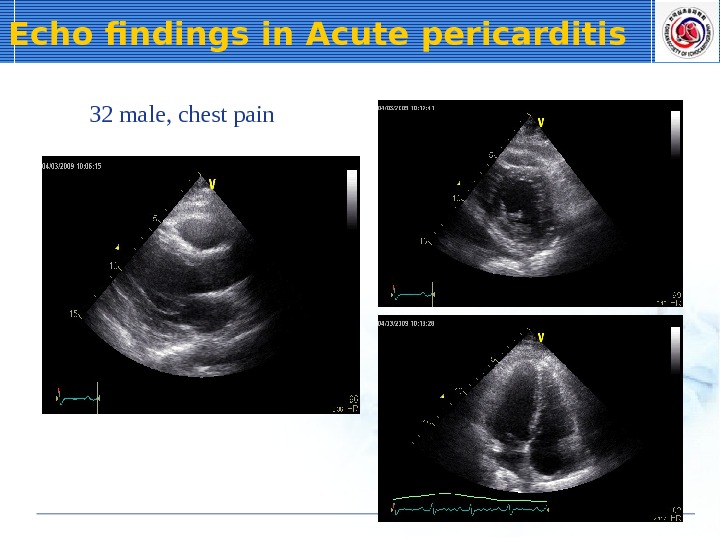
32 male, chest pain. Echo findings in Acute pericarditis
Cardiac tamponade Pericardial effusion with cardiac compression fatal rapid diagnosis is important Pathophysiology intrapericardial pressure increase intracardiac pressure increase limitation of ventricular filling reduction of cardiac output Etiology malignancy, idiopathic, uremia
Pathophysiology
dilated jugular vein, hepatomegaly paradoxical pulse: hallmark of tamponade constriction, RCM, COPD, asthma tachycardia, remote heart sound CXR & ECG: c/w pericardial effusion Echo. CG: confirmatory diagnosis pericardial effusion, diastolic RV collapse Clinical features
Electrical alternans
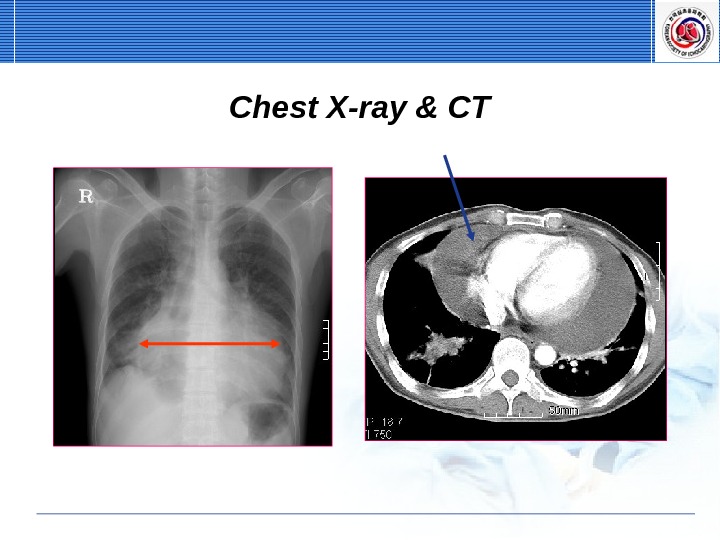
Chest X-ray & CT
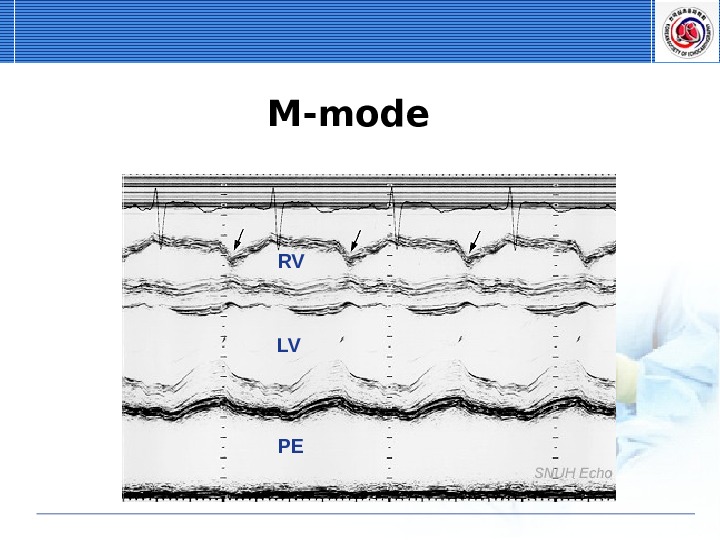
M-mode RV LV P
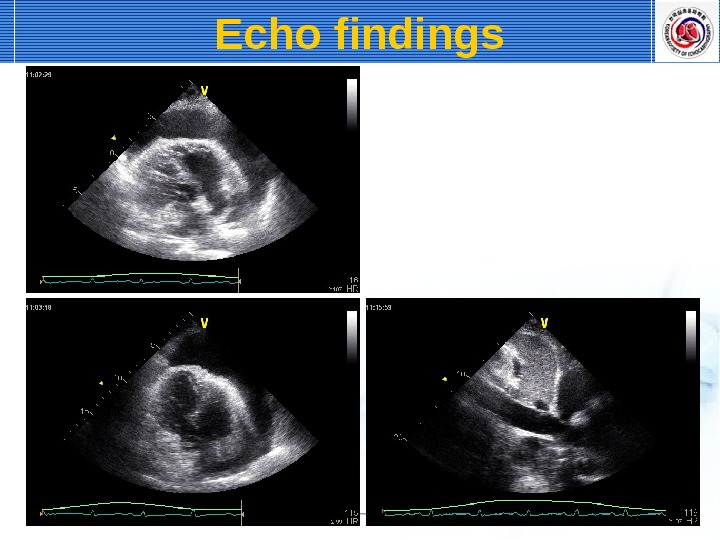
Echo findings
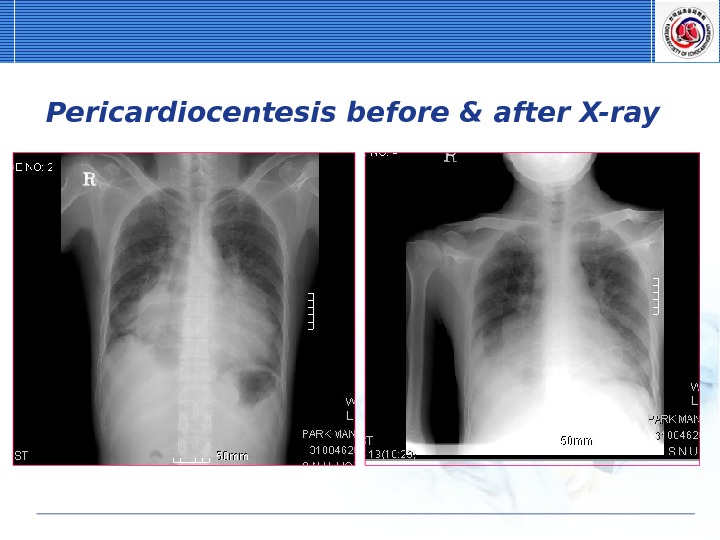
Pericardiocentesis, pericardiotomy
Pericardiocentesis before & after X-ray
Constrictive pericarditis Definition Pericardial fibrosis or calcification due to pericardial inflammation or complication cause restriction of ventricular relaxation Etiology unknown, tuberculosis, radiation, cardiac surgery, uremia, viral, neoplastic, purulent
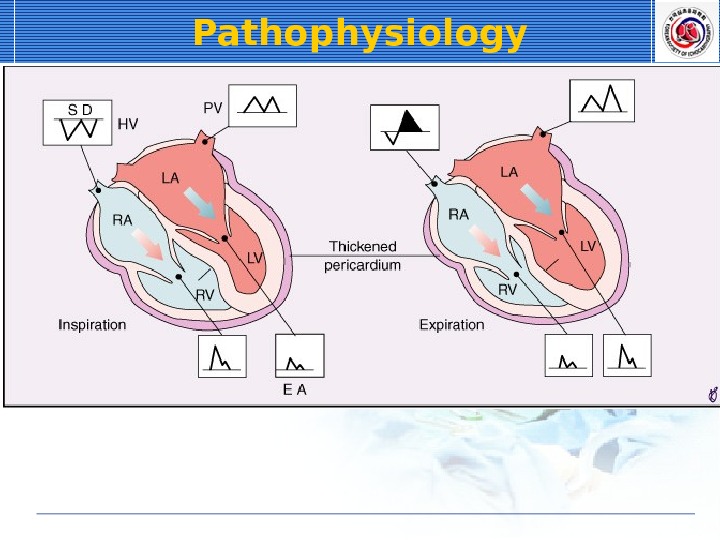
Pathophysiology
Constrictive pericarditis Pathophysiology chronic infl. , thickening, fibrosis, calcification constricts cardiac chambers diastolic dysfunction systemic venous pooling, low cardiac output Inspiration: MV flow velocity↓ Expiration: MV flow velocity ↑ Expiration: HV flow reversal ↑
systemic venous congestion edema, ascites, hepatomegaly JVP : prominent y descent, Kussmaul’s sign pulmonary venous congestion dyspnea, cough, orthopnea pulmonary edema: never occur low cardiac output: fatigue, weakness diastolic pericardial knock Clinical features
CXR pericardial calcification (only in half), pleural effusion, pulmonary congestion, LA enlargement ECG: low QRS, LAE, atrial fibrillation Echo. CG pericardial thickening, atrial dilation characteristic Doppler findings CT or MRI: pericardial thickening, calcification Clinical findings
Two-dimensional echo — pericardial thickening & calcification — can show evidence of right-sided pressure overload such as atrial septal shifting to the left with inspiration or dilated inferior and SVC and hepatic veins M-mode — septal bouncing & LV posterior wall flatening at diastolic phase — IVC plethora — non-specific Echo findings
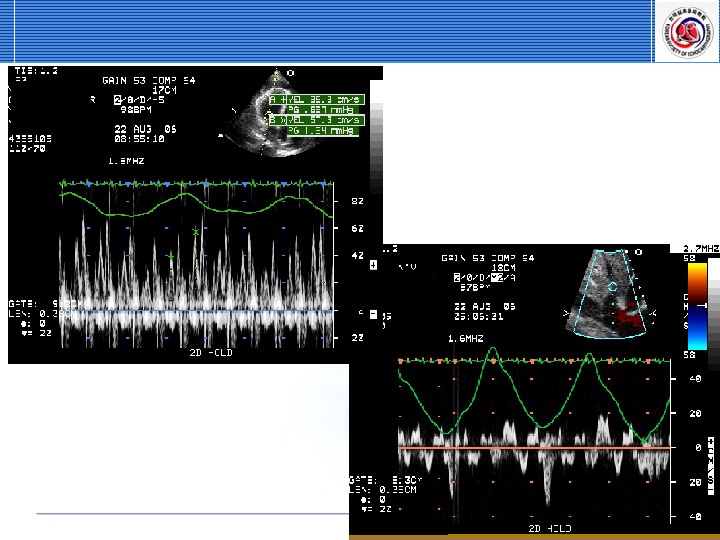
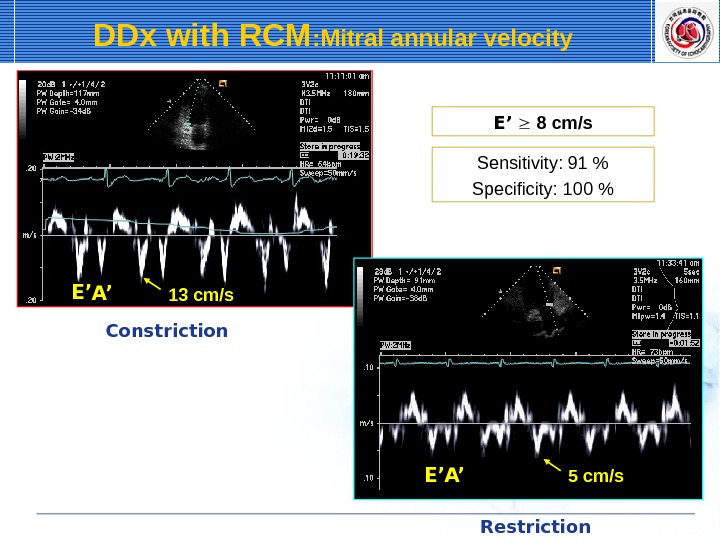
Doppler echo — provides important hemodynamic information — early rapid diastolic filling E (for early filling), A (for atrial filling) waves ① shortened durations ② increased velocity ③ rapid decelerations from their peak velocity ↓ ④ with inspiration & ↑ with expiration (≥ 25%) — Early annular tissue velocity 시시 (by TDI) E/A ration >1. 5 & E’ > 7~8 cm/s 시 시시 RCMP 시 시시시 Echo findings
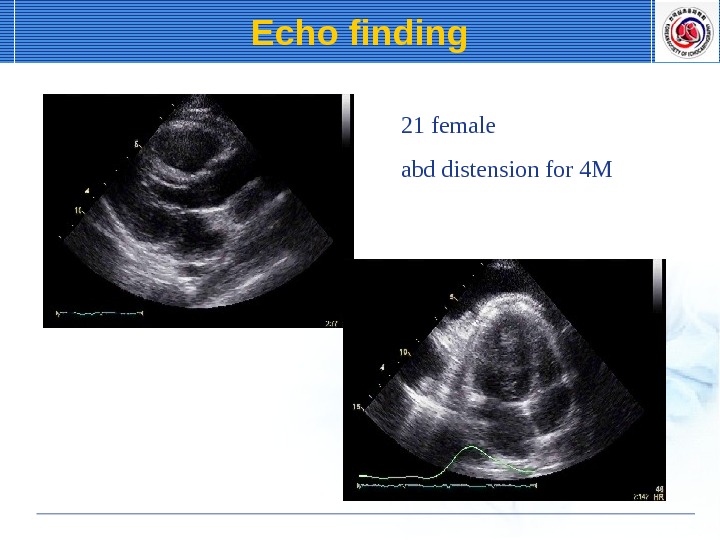
21 female abd distension for 4 MEcho finding
Doppler echo finding E A 0. 8 1. 2 Inspiration Expiration. MV inflow pattern HV flow pattern
E’ A’ 13 cm/s E’ A’ 5 cm/s E’ 8 cm/s Sensitivity: 91 % Specificity: 100 %DDx with RCM : Mitral annular velocity Constriction Restriction
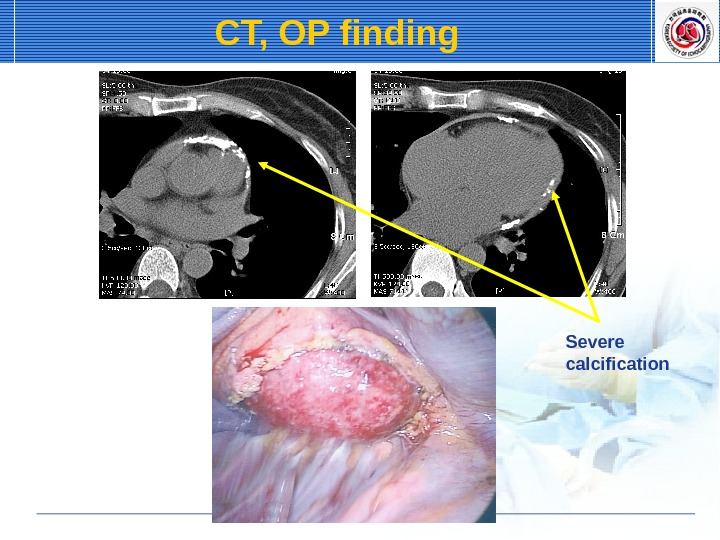
CT, OP finding Severe calcification